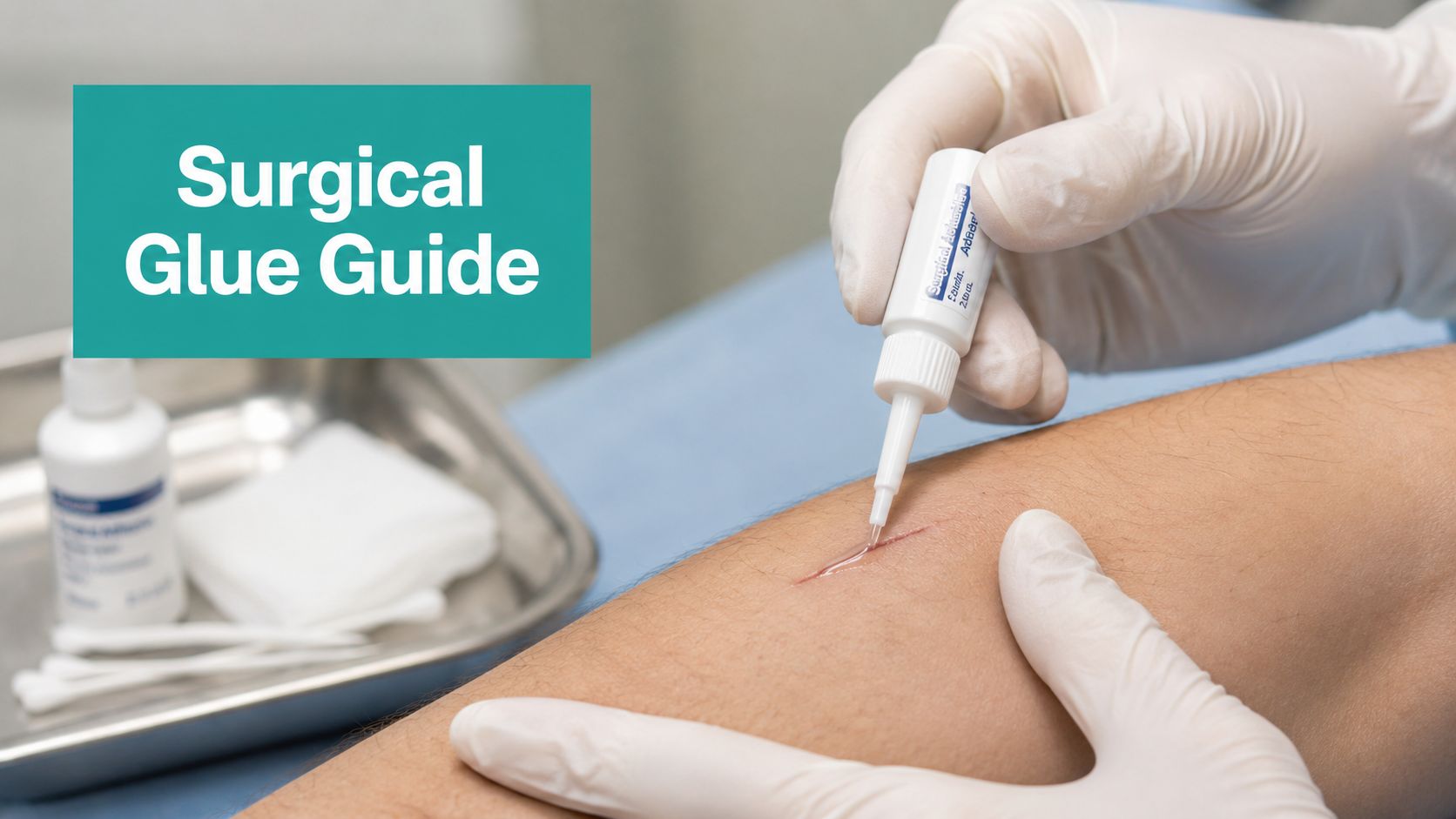
The most misleading advice about surgical glue for cuts is the idea that it's a simple “suture-free” upgrade. It isn't. It's a selective closure method with very clear mechanical limits, and most failures come from ignoring those limits rather than from the adhesive itself.
That matters in wound care, urgent care, dermatology, podiatry, and mobile practice. If you use glue on the wrong wound, you buy yourself dehiscence, callbacks, add-on documentation, and sometimes a denied claim because the chart never explained why adhesive closure was chosen in the first place. If you use it on the right wound, with a dry field and disciplined technique, it can be fast, clean, and very well tolerated.
The Reality of Surgical Glue for Cuts
Cyanoacrylate adhesives are not a stronger suture alternative. They provide only about 10% of the tensile strength of sutured wounds, which is why they fail more often when clinicians use them on wounds over 3 cm or in high-tension areas such as joints. In randomized trials, dehiscence occurs in 8 to 12% of glue-only closures versus 3 to 5% with sutures in low-tension wounds, and up to 25% in high-tension zones according to DermNet's review of topical skin adhesives.
That single fact should reset how you think about surgical glue for cuts. The right comparison isn't “glue versus sutures.” The comparison is “glue for the correct wound versus glue for the wrong wound.”
Practical rule: If the skin edges want to spring apart when you let go, glue alone probably isn't your closure.
In clinic, the best glue closures are boring. Short, clean, superficial, low-tension wounds. Dry field. No contamination. No active oozing. Edges come together easily and stay together with light fingertip control. Those are the cases where adhesives shine.
The trouble starts when convenience drives the decision. A mobile patient with a wound across a moving joint. A diabetic foot wound with depth and repetitive shear. A laceration with irregular edges and persistent bleeding. Those are not “make it work” situations. They're the reason many clinicians end up mistrusting a tool that performs well when used with discipline.
For teams trying to standardize closure choices, this is the same mindset behind evidence-based wound care practices. Match the intervention to the wound biology and the mechanical environment. Glue works. Overconfidence doesn't.
Wound and Patient Selection Criteria
The fastest way to improve outcomes with surgical glue for cuts is to stop thinking about the adhesive first and start with wound selection.

Start with the wound, not the product
The ideal adhesive candidate is a fresh, clean, superficial, low-tension wound with edges that approximate easily. If you have to fight the wound to line it up, you're already outside the sweet spot.
Age matters. A wound that's older than the usual early window is more likely to fail if you seal it with glue, especially if contamination is in the picture. Heavy bioburden, delayed presentation, irregular edge quality, and deeper tissue involvement all push the wound away from adhesive-only closure and toward another strategy.
For chronic wound clinicians, the biggest mistake is extending acute laceration thinking into ulcer care. Adhesives are not designed to rescue a poorly offloaded, high-stress lower extremity wound. They're not a shortcut around proper debridement planning, edema control, pressure redistribution, or layered closure principles.
Where glue fits and where it doesn't
Superficial wounds are where adhesives make sense. Partial-thickness skin edge closure in a low-tension setting is very different from trying to close a deeper, multi-layer defect that still has dead space, undermining, or shear.
A useful mental screen:
| Adhesive Suitability Checklist | Use Surgical Glue When… | Avoid Surgical Glue When… |
|---|---|---|
| Depth | The wound is superficial and doesn't require layered closure | The wound is deep, multi-layer, or needs buried support |
| Tension | Edges meet easily and remain approximated with light support | Edges separate, gape, or sit across a joint or mobile surface |
| Cleanliness | The wound is clean and not heavily contaminated | The wound is contaminated, older, or clinically unsuitable for sealing |
| Location | The site is relatively low-stress and dry | The site is high-tension, moist, or subject to repetitive motion |
| Wound type | Linear cut with predictable edges | Bite, puncture, crush, irregular tear, or chronic ulcer scenario |
| Lower extremity risk | Superficial, selected low-stress wound only | Wagner grade 2 or higher foot ulcer, web space, Achilles region, or other high-stress area |
If you're documenting a diabetic foot wound with depth, exposed deeper structures, tunneling, or ongoing exudate management, you're no longer talking about an adhesive-first problem.
Patient factors that change the decision
Wound selection and patient selection are tied together. A patient who can't follow aftercare instructions, keeps the area wet, or applies ointments to everything may not be a good adhesive candidate even if the wound itself looks acceptable.
The lower extremity deserves extra caution. 2-octylcyanoacrylate has higher tensile strength and flexibility than N-butyl variants, but inappropriate selection for Wagner grade 2+ foot ulcers or deep, multi-layer injuries leads to dehiscence in 15 to 20% of cases, as described in the PMC review on skin adhesives and closure strength. That aligns with what many of us see in practice. The failure isn't mysterious. The wound needed more mechanical support than glue could provide.
Patient skin quality also matters. Friable skin can benefit from avoiding multiple needle passes, but fragile skin isn't a reason to ignore tension. If anything, it means you need an even cleaner closure plan.
Pre-Application Wound Preparation
Most adhesive failures are set in motion before the adhesive tip ever touches the skin.
Dryness and hemostasis are non-negotiable
For surgical glue for cuts, the field has to be clean, dry, and quiet. That means irrigation, removal of visible debris, and control of bleeding before you open the adhesive. A little oozing is not harmless. Blood and moisture interfere with polymerization, let glue track where it shouldn't go, and weaken the surface bond.
If I'm dealing with a small wound that looks appropriate for adhesive closure, I slow down here. Direct pressure first. If needed, topical hemostatic support within your protocol. Then reassess the edge quality and the periwound. Maceration, heavy serous drainage, and persistent capillary ooze should all make you hesitate.
Debridement and edge preparation
Minor edge freshening may be reasonable when you need a cleaner, better-apposed surface. In wound care language, that's a very different scenario from extensive debridement. Once you're into meaningful devitalized tissue removal, undermining assessment, or a debridement service such as CPT 11042 to 11047, you should be asking whether adhesive-only closure still makes clinical sense.
Use your normal wound assessment discipline:
- Periwound review: Look for maceration, erythema, callus, friability, and signs of adhesive intolerance.
- Exudate check: Minimal drainage is one thing. Ongoing serous, serosanguineous, or purulent output is another.
- Infection screen: If the wound is clinically infected, glue isn't the answer. A structured review of how to tell a wound is infected helps junior clinicians avoid sealing over a problem they should be treating.
The cleanest note in the world won't save a bad closure choice. Preparation drives the result.
The field should look boring before closure
Before adhesive application, I want no active bleeding, no shine from residual fluid, no visible gap under the edge, and no need for forceful traction to hold the wound together. If that checklist isn't met, stop and change strategy. That decision prevents a lot of avoidable dehiscence.
The Correct Application Technique
Application should look controlled and almost uneventful. Fast isn't the same as rushed.

What good technique looks like
Approximate the wound edges first. Use fingers or forceps to bring them together precisely, with slight eversion if possible. The adhesive goes over the approximated skin edges, not down into the wound bed. If glue gets inside the wound, you've turned a surface bridge into a foreign material problem within the closure plane.
The best closures usually start in the middle, then extend outward as alignment is maintained. That prevents the common drift you see when one edge gets anchored crooked and the rest of the wound follows.
The method itself should be thin and deliberate. A thin film of 0.5 to 1 mm across the approximated edges reduces closure time to 1.50 ± 0.63 minutes versus 2.23 ± 0.66 minutes for sutures, with equivalent cosmetic outcomes and 4.73/5 scar satisfaction scores, according to Net Health's summary of tissue adhesive technique and outcomes.
Common technical errors
A lot of residents make the same three mistakes:
- They apply too much glue. Thick layers crack, run, and create a brittle bridge.
- They stop controlling the edges too early. The wound shifts before the polymer sets.
- They let glue seep into the wound. That increases irritation and undermines proper healing.
Keep the adhesive superficial. Think bridge, not filler.
I prefer multiple light passes over one heavy coat if the wound needs a bit more surface reinforcement. Each layer should stay thin. The goal is a neat external film that holds already-approximated skin edges in place.
Where speed helps and where it hurts
The time advantage is real, especially in a busy clinic or procedure day. But speed only helps after the wound has earned adhesive closure through proper selection and prep. If you use glue to save time on a wound that should have been layered, offloaded, or sutured, you lose that time later in rechecks, dressing changes, and chart addenda.
Post-Procedure Care and Failure Analysis
Closure isn't finished when the adhesive dries. The outcome now depends on patient behavior, wound mechanics, and the details you either handled correctly or missed.

What the patient needs to hear
Patient instructions should be short and blunt. Keep the area dry initially. Don't scrub it. Don't pick at the film. Don't apply ointments, creams, petroleum jelly, or topical antibiotics over the adhesive. Let it peel off naturally.
That last point gets missed constantly. Patients see a wound and reach for ointment by reflex. If you don't give a clear warning, some of them will dissolve your closure for you.
Why some glue closures do very well
When the wound is selected correctly and the closure is done well, adhesives can perform better than many clinicians expect. In a lower extremity dermatologic surgery cohort, 2-octyl cyanoacrylate was associated with a 62.40% relative risk reduction in culture-positive surgical site infections compared with the pre-adoption era, and patients often report higher satisfaction because the procedure is faster and there's no removal visit, as summarized by Dermatology Advisor's report on lower extremity outcomes with 2OCA.
That doesn't mean glue is safer in every setting. It means careful use in the right wound can be very effective.
Failure analysis at the bedside
When a glue closure fails, I usually trace it to one of four causes:
- Bad tension judgment: The wound should never have been closed with adhesive alone.
- Poor field control: Residual bleeding or moisture prevented a stable seal.
- Wrong wound biology: Contamination, delayed presentation, or active infection was underestimated.
- Aftercare failure: The patient got the site wet early, rubbed it, or applied ointment.
A smaller group develops contact irritation. That tends to show up as localized itching, erythema, or swelling around the film rather than a deeper closure problem. Distinguish that from cellulitis and from simple mechanical edge separation.
A reopening wound is usually a planning error before it's a product problem.
For lower extremity and mobile wound practice, look hard at offloading and repetitive shear. A wound can look acceptable at rest and still fail once the patient starts walking, transferring, or flexing through the area all day.
Documentation and Coding for Adhesives
If you want to get paid without avoidable friction, document the closure like you expect an auditor to read it. Because sometimes they will.
What has to be in the note
For adhesive closure, vague charting is what gets practices into trouble. “Wound glued” is not a defensible procedure note. Payers want the same fundamentals they'd expect for any repair decision, and the chart has to explain medical necessity, technique, and aftercare.
Payer auditors frequently deny claims for wound glue closure if the note doesn't document that bleeding was controlled via pressure before application, doesn't confirm the wound edges were clean, dry, and aligned, and doesn't explicitly state that no topical antibiotics or petroleum jelly were applied, based on the documentation guidance summarized by SubQ-it on surgical glue charting pitfalls.
Use language like this in your procedure note:
- Site and size: Record exact location and measured length.
- Wound characteristics: State superficial depth, contamination status, edge quality, and tension assessment.
- Hemostasis: Document that bleeding was controlled before adhesive contact.
- Preparation: Note cleansing, any limited debridement, and that the skin surface was dry.
- Closure method: “Wound edges well approximated and aligned. Tissue adhesive applied topically over approximated edges.”
- Aftercare: Document that the patient was told to avoid ointments and petroleum products, avoid soaking or scrubbing, and allow natural peeling.
Coding judgment matters
In US billing, this usually lives within simple repair logic when the wound qualifies as a simple superficial closure. If you also performed debridement, be careful. Don't blur a distinct debridement service with a minor edge refresh that was merely part of wound prep. If the visit involved a chronic wound with depth, devitalized tissue, exudate management, Wagner staging, and debridement coding such as 11042 to 11047, the chart needs to clearly separate what was treated, what was closed, and why.
That's also where secure documentation systems matter. Practices handling wound photos, measurements, and legal requests need workflows that respect privacy and chain of access. Teams reviewing broader compliance processes may find cybersecurity for legal HIPAA regulations useful, especially when records move across clinical, billing, and legal channels.
What surveyors and auditors actually look for
They look for internal consistency. If the wound was dry and suitable for adhesive closure, your note shouldn't also describe heavy exudate or persistent bleeding. If the wound crossed a high-motion area, your note should justify why adhesive was still appropriate or explain what deeper support offloaded tension. If you chose glue to avoid suture removal in a straightforward low-tension wound, say so plainly.
Clean claims start with notes that sound like the clinician examined the wound.
EkagraHealth AI helps wound care teams turn that kind of clinical thinking into clean, defensible documentation. It listens during the encounter, drafts the note, supports CPT and ICD-10-CM mapping, and helps get claims out the door without forcing clinicians to spend their evening rebuilding the visit from memory. If your practice is tired of charting more than treating, EkagraHealth AI is worth a look.
