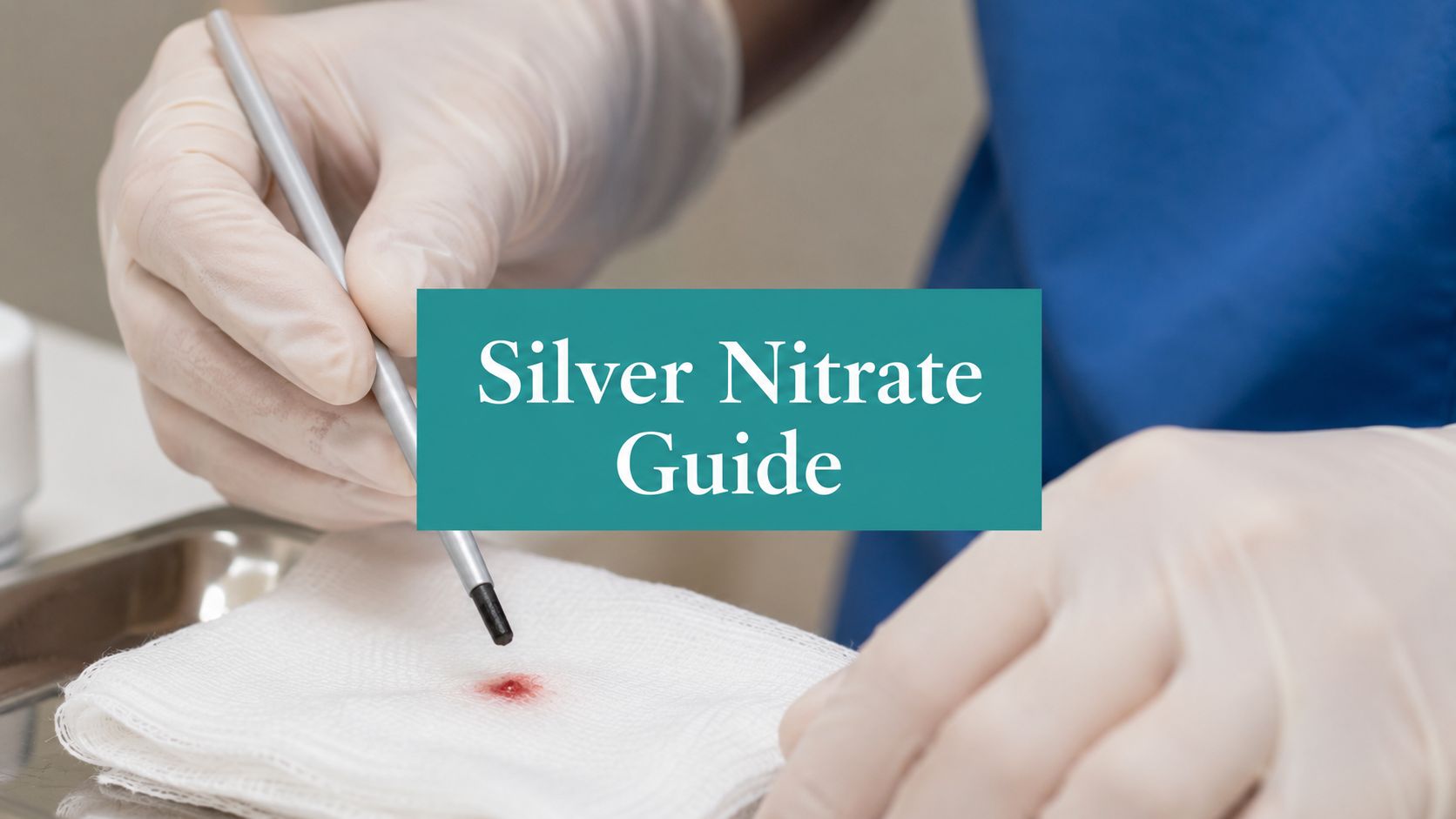
You've probably had this visit already today. The wound is otherwise moving in the right direction, bioburden is controlled, offloading is reasonable, edema is being addressed, and then one stubborn rim of hypergranulation or rolled edge keeps the surface from closing. Someone reaches for a silver nitrate stick, applies it, and the tissue darkens. Clinically, that part is easy.
What usually goes wrong happens afterward. The note says “granulation treated with silver nitrate,” the claim goes out with weak diagnosis support, no tissue characterization, no frequency rationale, and then the denial lands. That's the part most quick clinical explainers skip.
Used well, silver nitrate is a precise tool. Used casually, it burns healthy tissue, underperforms in wet wounds, and creates documentation problems that are completely avoidable.
Table of Contents
- Indications and Contraindications A Realistic Assessment
- The Application Protocol From Prep to Periwound Protection
- Managing Complications and Complex Wound Environments
- The Documentation and Coding That Justifies Treatment
- Post-Application Care and Clear Patient Instructions
- Frequently Asked Questions
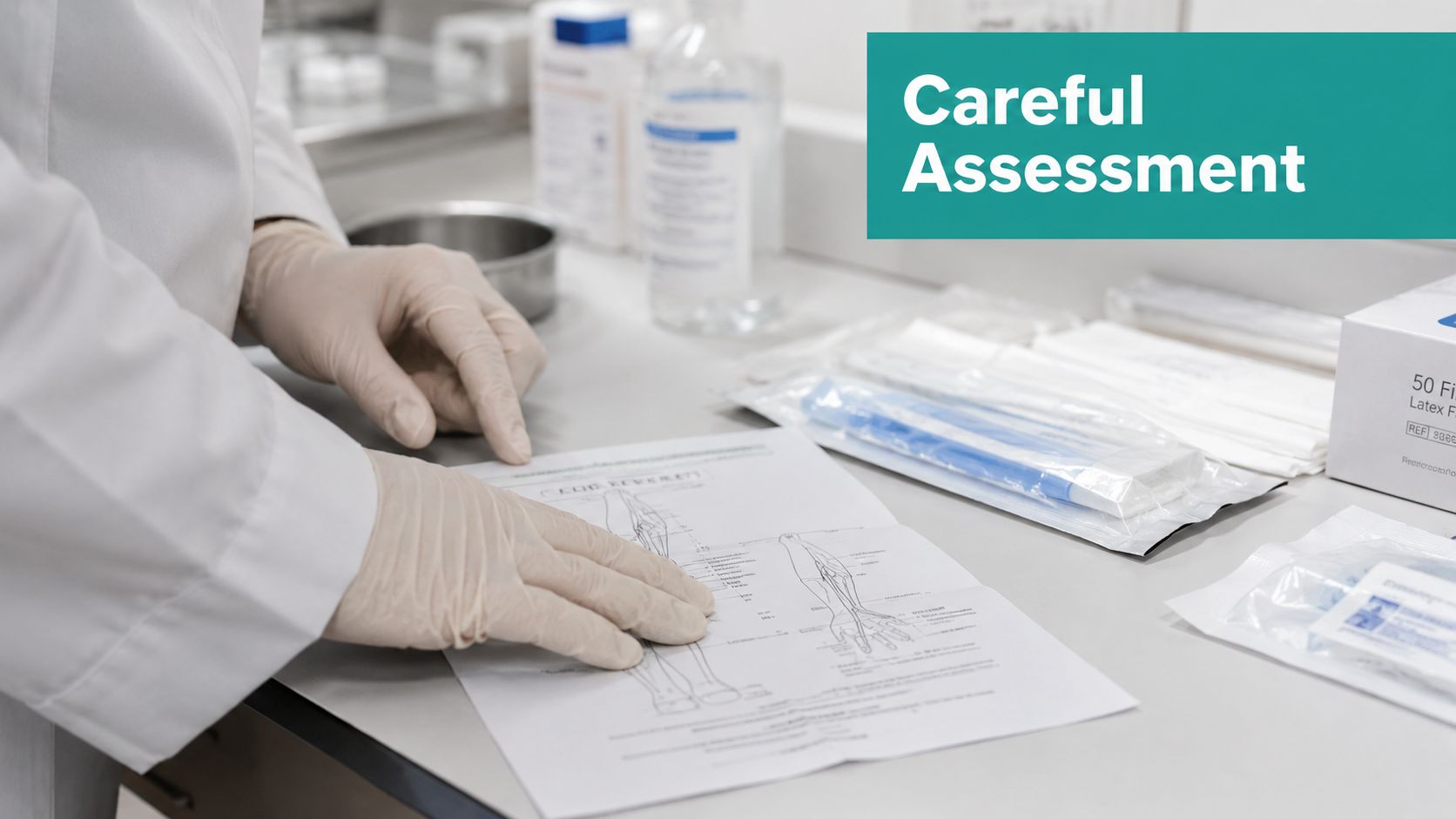
Indications and Contraindications A Realistic Assessment
A common wound clinic scenario looks like this: the ulcer is cleaner, bioburden is under better control, exudate is no longer flooding the dressing, and healing still stalls because a mound of friable tissue keeps growing above the wound surface. Silver nitrate has a place there. It is a targeted chemical cautery option for a narrow set of problems, and the note needs to show that narrow fit if you expect the treatment to hold up clinically and financially.
Where Silver Nitrate Actually Fits
In wound care, the best indications are specific and visible at the bedside:
- Hypergranulation tissue rising above the wound plane and interfering with epithelial advance
- Rolled or non-advancing edges when chemical cautery is part of the plan to disrupt that stalled edge
- Minor superficial bleeding from friable tissue after routine manipulation or dressing removal
That is the practical lane. If you want a quick visual refresher on the difference between healthy granulation and tissue that has become a barrier to closure, this review of granulation tissue definitions and healing context is useful.
The decision should stay tied to the actual wound problem in front of you. Silver nitrate works for excess superficial tissue and small surface bleeders. It does not correct depth, dead space, undermining, ischemia, pressure, high bacterial burden, or moisture imbalance.
That distinction matters for documentation. A claim is easier to defend when the note states the target tissue, why it is impeding progress, and why chemical cautery was chosen instead of debridement, hemostatic pressure, or simple local wound care. If the chart just says "silver nitrate applied," expect pushback.
The evidence base for hemostatic use is also narrower than many clinicians assume. A wound care review notes that silver nitrate is used for small-volume bleeding and hypergranulation, but also states that an NCBI rapid review found no comparative clinical trials, no cost-effectiveness studies, and no evidence-based guidelines meeting criteria for topical silver nitrate in hemostasis, as summarized in this WoundSource review on silver nitrate sticks.
Where It Does Not Fit
Silver nitrate is not a substitute for debridement. If the wound bed is necrotic, fibrotic, heavily sloughed, or clearly requires selective or sharp debridement, treat that problem directly and document it directly. Using a cautery stick on the wrong tissue is poor wound management and weak billing support.
Avoid silver nitrate when precision is limited or tissue injury would carry more risk than benefit:
- Near the eyes
- On brisk bleeding or a suspected arterial source
- On larger treatment areas where chemical spread is hard to control
- On healthy surrounding skin that cannot be protected
- On suspicious lesions that need diagnosis before destruction
- On wounds where untreated infection, ischemia, or another primary driver is the reason healing has stalled
The primary failure point in practice is usually not the stick. It is case selection. If the wound has a systemic or structural problem, silver nitrate may darken tissue and create the appearance of treatment without changing the trajectory of healing.
Document contraindications and failed alternatives when they affect the decision. If the patient has pain sensitivity, fragile surrounding skin, repeated recurrence of hypergranulation, or a wound etiology that makes recurrence likely, put that in the note. That kind of detail supports medical necessity and shows you used judgment rather than a routine reflex.
The Application Protocol From Prep to Periwound Protection
You can lose the whole visit before the stick ever touches tissue. The common failure is not the chemistry. It is poor setup, vague targeting, and a note that never explains why chemical cautery was the right choice that day.

Set Up the Field Before You Touch the Stick
Start with tissue identification. If the target is friable hypergranulation above the wound plane, or a small superficial bleeding point, silver nitrate can be a reasonable bedside treatment. If you are looking at slough, necrosis, adherent fibrin, or a wound that needs debridement, change course. That decision belongs in the chart because it supports why you performed cautery instead of another procedure.
Preparation should be deliberate, not rushed:
- Cleanse the wound so you can see the true margins and the tissue you intend to treat.
- Blot excess moisture to improve control. An overly wet field invites runoff onto healthy skin.
- Protect the periwound with a barrier ointment or comparable skin protectant around the target tissue.
- Explain what the patient may feel. A brief burning sensation is common. Escalating pain means stop and reassess.
Technique stays simple when the field is controlled. Cleanse. Isolate. Protect. Then apply the stick to the intended tissue with a light rolling motion. If the wound surface is too dry to activate the tip, moisten it with sterile water, not saline. As noted earlier, treated tissue often turns gray or dark after contact. For the broader care plan around the procedure, the surrounding dressing choice still matters, especially in wounds with drainage or friction risk. This guide to wound healing dressings and dressing strategy is useful when deciding what should cover the site after cautery.
Apply It With Control, Not Force
Pressure is a mistake. Silver nitrate works by contact time and precision.
Roll the applicator over the hypergranulation or pinpoint bleeding area. Keep the pass short. Watch the tissue response. Stop once you have the effect you need. Repeated scrubbing usually buys you more tissue injury, more pain, and a harder follow-up note to defend.
A few details make a visible difference in practice:
- Dry wound surface: moisten the tip with sterile water
- Moist wound surface: the existing moisture may be enough to activate the applicator
- Do not use saline on the tip: it can interfere with the treatment effect
- Expect discoloration: the tissue may darken immediately or later the same day
- Stop for significant pain: do not force another pass just to make the endpoint look more dramatic
A single applicator is often enough for a straightforward hemostatic treatment. If you need repeated sticks on a routine wound, reconsider the wound environment first. Heavy exudate, poor exposure, bulky tissue, or a wrong target usually explain the struggle better than "insufficient silver nitrate." That observation also belongs in the note because it shows clinical judgment rather than routine repetition.
Protect the Periwound and Manage Misfires
Periwound protection is where experienced technique shows. The target should be isolated before activation. Once the tip gets too wet, control drops fast and healthy skin pays for it.
Use a barrier ring or ointment around the treatment site. Keep dry gauze ready. If the chemical contacts intact skin by mistake, clean the area promptly. Guidance from AboutKidsHealth on silver nitrate use notes that saline can be used afterward to neutralize accidental contact with healthy tissue.
The avoidable errors are consistent:
- Over-wetting the applicator and letting the agent run
- Treating the whole wound surface instead of the raised or bleeding tissue only
- Ignoring patient pain response
- Using silver nitrate where debridement or another intervention is the correct procedure
If payment is part of the goal, document the setup as clearly as the application. Note the target tissue, the periwound protection used, patient tolerance, the endpoint achieved, and why cautery was chosen instead of debridement or simple pressure. That level of detail is what separates a defensible procedure note from a claim that looks routine, unsupported, or duplicative.
Managing Complications and Complex Wound Environments
A common failure looks like this. The wound has heavy drainage, the hypergranulation is obvious, someone reaches for silver nitrate anyway, and the tissue barely changes while the surrounding skin ends up irritated. The problem is usually not the stick. The problem is timing, wound conditions, or a poor match between the clinical goal and the treatment chosen.
Complications in this setting are usually predictable and preventable. They also need to be documented with enough specificity that a repeat treatment, a change in plan, or a denied claim can be defended later. If silver nitrate was attempted in a difficult wound and did not achieve the expected endpoint, that belongs in the note.
The Common Failures Are Usually Technique or Wound-Selection Problems
| Problem | What usually caused it | What to do |
|---|---|---|
| Periwound chemical irritation | Inadequate skin protection or runoff from an over-wet tip | Stop treatment, cleanse the area, reassess skin protection before any future attempt |
| Tissue staining | Expected effect of cautery or unintended contact outside the target | Document expected discoloration so it is not later misread as necrosis |
| Over-cauterized surface | Contact time too long or repeated passes on already-injured tissue | Stop and reassess. More silver nitrate is rarely the answer once the surface has already been injured |
| Poor response | Wrong indication, heavy moisture, slough blocking contact, or friable tissue that needs a different approach | Correct the wound environment first, then decide whether chemical cautery still makes sense |
Pain limits treatment more often than clinicians admit. If the patient is pulling away, reporting sharp burning, or refusing a second pass, document that clearly and stop. A forced application usually worsens trust, reduces follow-up tolerance, and leaves you with a weak note if the result is poor.
Heavy Exudate Changes What Silver Nitrate Can Do
Silver nitrate works poorly in a flooded field. In a heavily draining wound, ongoing moisture can dilute the chemical before it cauterizes the target tissue. Slough, biofilm, and constant serous output can also block contact. In practice, that means the clinician may use multiple sticks, see little or no gray-black tissue change, and still leave the visit with an irritated margin and no meaningful reduction in hypergranulation.
That pattern is especially common in deeper diabetic foot wounds, pressure injuries, and cavity wounds with persistent drainage. On those days, moisture control is the treatment priority. Chemical cautery is secondary.
Use a simple decision process before you commit:
- Reduce the moisture burden first if exudate is obscuring the target
- Cleanse and remove surface material that prevents contact, if appropriate within the treatment plan
- Limit treatment to the discrete raised or bleeding tissue, not the whole wound bed
- Stop if there is no expected tissue response after a reasonable attempt
- Document why silver nitrate was deferred, abbreviated, or unsuccessful
That last point matters for payment. If a wound is too wet for effective cautery and you proceed anyway, the note can read like a routine, unsupported repeat service. If you document heavy exudate, failure to achieve the expected endpoint, the reason further application would increase tissue trauma, and the revised plan, the record shows clinical judgment. That is the difference between a defendable procedure history and a pattern that invites payer scrutiny.
Complex Wounds Need a Different Threshold for Aborting the Attempt
In complex wounds, the right decision is often to stop. Do that when the tissue is not clearly hypergranulation, when the wound bed is unstable, when pain escalates quickly, or when bleeding suggests you are treating beyond the intended superficial target.
The note should reflect the trade-off. Record what made the wound environment unfavorable, what endpoint was or was not achieved, and what alternative plan was selected instead. That level of detail supports continuity of care and helps with avoiding billing compliance pitfalls, especially when repeated procedural treatment is being questioned.
If your team sees repeated denials on these encounters, align the procedure note with diagnosis specificity and medical necessity from the start. A practical reference for pairing wound documentation with procedure support is this guide to ICD-10 and CPT coding for wound care services.
The Documentation and Coding That Justifies Treatment
Practices lose money because the procedure gets done correctly, but the note is vague, the diagnosis support is weak, and repeat frequency is never justified. Payers don't infer clinical reasoning from a one-line procedure note.
What the Note Must Say
If you use silver nitrate for hypergranulation or epibole, the note should identify the tissue problem with enough specificity that another clinician, auditor, or payer reviewer can understand why chemical cautery was chosen.
Document these elements clearly:
- Target tissue: hypergranulation, proud flesh, epibole, or superficial bleeding point
- Location: exact wound or site treated
- Clinical reason: blocking epithelial advancement, recurrent friable bleeding, persistent raised tissue
- Wound context: exudate level, periwound condition, infection signs if present or absent
- Prior conservative management: dressing changes, moisture management, offloading, barrier protection, local care
- Response during treatment: tissue darkened, hemostasis achieved, patient tolerance, procedure stopped early if painful
- Planned frequency: and why that interval is appropriate
The coding challenge is real. Clinicians often struggle to pair CPT codes such as 17000 and ICD-10-CM codes such as L98.8 for hypergranulation with a defensible frequency statement, and a 2024 CMS manual update highlighted that vague notes on “granulation treated” without specific tissue characterization and frequency rationale were associated with 30% higher claim rejection rates for wound care services. That point is included in the verified documentation guidance you provided, and it should shape how every repeat application is charted.
How to Pair the Procedure With Diagnosis and Frequency
The diagnosis needs to reflect the tissue abnormality you treated. If the note says “chronic wound care performed” and never identifies hypergranulation or epibole, the coding support is weak from the start.
Common pairings in practice include:
- CPT 17000 when the service is documented as chemical ablation or destruction in the appropriate clinical context
- CPT 97597/97598 only when selective debridement is also performed and separately supported by the documentation
- ICD-10-CM L98.8 when documenting other specified skin disorder such as hypergranulation, if that matches the encounter
- ICD-10-CM L98.9 when epibole or abnormal tissue change is being documented more generally and that code selection is medically appropriate under payer policy
Don't use debridement codes as a workaround when no debridement occurred. Auditors look for mismatches between the wound description, tissue removed, instrument used, depth documented, and the code submitted.
For teams trying to tighten denials and internal audit risk, this article on avoiding billing compliance pitfalls is worth reading alongside your wound-specific policies. The main lesson applies here too: vague documentation gets interpreted against you.
A Practical SOAP Framework
A defensible note doesn't need to be long. It needs to be specific.
“Hypergranulation treated” is not a billable story. It's a fragment.
Use a structure like this:
Subjective
- Patient reports persistent drainage, intermittent minor bleeding with dressing changes, or pain from raised tissue if applicable.
- State whether conservative local care has failed to flatten the tissue.
Objective
- Wound location and relevant classification if already established
- Tissue finding: hypergranulation above skin plane, epibole at margin, friable superficial bleeding point
- Exudate type and amount
- Periwound status
- Whether there are features suggesting the need for another intervention instead
Assessment
- State why silver nitrate is appropriate for this visit
- State why sharp debridement was not the primary intervention, if that distinction matters
Plan
- Silver nitrate applied to the target tissue with periwound protection
- Number of applications or sticks used, if relevant to the record
- Immediate tissue response
- Patient tolerance
- Follow-up interval and frequency rationale
A separate procedural line helps. So does linking the treatment to a diagnosis code set that reflects the tissue problem rather than only the underlying ulcer.
If your clinicians need support keeping the coding logic aligned with the clinical note, this reference on ICD-10 and CPT code mapping in wound care is the kind of resource that helps reduce preventable mismatches.
Post-Application Care and Clear Patient Instructions
Silver nitrate isn't a one-visit magic trick. Hypergranulation often needs repeat treatment, and that plan should be intentional.
Follow-Up Planning for the Clinician
For hypergranulation or epibole, some protocols repeat treatment daily to three times per week until the tissue is level with surrounding skin, with a practical ceiling of up to 14 days before escalation is advised, based on the verified application guidance already noted earlier in the article. Another protocol for granulation tissue at tube or exit sites uses treatment every 2 days for up to 2 weeks, which shows the same basic principle: repeat treatment may be needed, but not indefinitely.
If the tissue isn't responding, stop reflexively reapplying silver nitrate and reassess:
- Is the wound too wet?
- Is pressure, friction, or device movement recreating the tissue?
- Is there untreated bioburden or inflammation?
- Does the edge need debridement instead of more cautery?
Simple Instructions You Can Hand to the Patient
Use plain language. Patients don't need a chemistry lecture.
- The treated tissue may turn gray or dark. That can be normal after this treatment.
- Keep the dressing in place as instructed. Change it only the way your clinician told you to.
- Don't scrub or pick at the treated area. Let the tissue settle.
- Call the clinic if pain becomes significant, if redness spreads, or if drainage suddenly worsens.
- Call if you have bleeding that doesn't stop with local pressure or if the area looks very different from what was explained.
Short, clear instructions prevent a lot of unnecessary panic calls and a lot of missed warning signs.
Frequently Asked Questions
Can I use silver nitrate on a suspicious lesion or bleeding mole
No. If the lesion is suspicious, diagnose it properly. Silver nitrate destroys surface detail and can delay the right workup.
Is one stick enough
For superficial hemostasis, several clinical references say one applicator is usually enough for one treatment. Moist wounds or bulky hypergranulation may require more than one stick. If you routinely need several, reassess the indication and moisture balance instead of assuming more is better.
What concentration are these sticks
The common wound care cautery stick is 75% silver nitrate and 25% potassium nitrate.
Should I moisten the tip with saline
No. If the wound is dry, moisten with sterile water. Saline can reduce effectiveness on the tip.
What if the patient says it burns badly
Stop. Pain is a practical endpoint. Significant burning means you need to reassess tissue selection, contact area, and whether that patient will tolerate further treatment.
Do silver nitrate sticks replace debridement
No. They are for precision cautery of selected superficial tissue problems. They do not replace proper debridement of a necrotic or nonviable wound bed.
If your team is doing the clinical part well but still losing time on charting, coding, and repeat-visit justification, EkagraHealth AI is built for exactly that gap. It helps wound practices document tissue findings, map CPT and ICD-10 logic, and get cleaner claims out without turning every silver nitrate application into a billing argument.
