You're in the room, glove on, dressing off, and the wound doesn't look like it did last week. Exudate is heavier. The edge is starting to roll. The patient says the foam kept slipping, and your usual absorptive option isn't in the supply closet today. That's the moment a static cheat sheet stops being enough.
Most dressing mistakes don't happen because the clinician doesn't know the categories. They happen because the wound changed, the setting changed, the patient changed, or the formulary got in the way. Then the note doesn't clearly connect the assessment to the product choice, so billing gets challenged later.
A useful wound dressing selection chart isn't a memorization exercise. It's a way to make a defensible decision under ordinary clinic pressure. You need something that helps you choose the best available dressing for today's wound, document why it was medically necessary, and know when to stop pretending a dressing is “still working” when the wound is telling you otherwise.
Stop Guessing Your Next Dressing
The fastest way to get into trouble is to choose the next dressing by habit. “This looks like a foam wound.” “We usually use hydrocolloid here.” “Let's keep doing what home health has been doing.” That kind of autopilot is how wounds stall.
A dressing choice should come from the wound you have today, not the wound you had two visits ago. In practice, that means reassessing exudate, tissue type, edge behavior, periwound condition, depth, and whether your goal is absorption, hydration, protection, filling dead space, or bioburden control. If one of those changes, the dressing may need to change too.
Practical rule: If your note shows a changed wound but an unchanged rationale, expect pushback from a payer and skepticism from any auditor reading the chart.
The practical problem is that dressing selection sits at the intersection of three pressures:
- Clinical need: The wound may need moisture donation, vertical absorption, protection of fragile granulation, or a filler that won't create pressure in a tunnel.
- Operational limits: Your formulary may be narrow, the patient may have limited caregiver support, and change frequency may matter more than unit price.
- Documentation burden: If you can't explain why this dressing was chosen over a simpler one, you've left the medical necessity argument unfinished.
Newer clinicians often want a single chart that says, “If wound A, use dressing B.” That isn't how this works. A wound dressing selection chart is useful only if it forces you to think in sequence. Assess first. Match function second. Confirm practicality third. Document the reason in language a reviewer can follow.
That's what keeps you from guessing.
Your Core Dressing Selection Framework
A sound wound dressing decision starts before you ever open the product drawer. The frame I trust most is the one built around Ovington's six assessment questions: what the wound needs, what the product does, how well it performs, what the patient needs, what is available, and what is practical. An expert-level wound dressing selection chart is dynamic, not static, and this assessment has to be repeated at every dressing change because wound needs evolve, as outlined by Wound Education Partners on Ovington's framework.

That sounds academic until you use it in clinic. Then it becomes very practical.
Ask what the wound needs first
Start with the wound, not the dressing brand category in your head. Does it need absorption, moisture, gentle coverage, dead-space filling, atraumatic removal, or antimicrobial management? A dry wound and a wet wound can both be “chronic lower extremity ulcers,” but they don't need the same thing.
A chronic wound framework also has to account for wear time, comfort, ease of use, debridement properties, and cost-effectiveness. If you want a good refresher on that evidence-based mindset, this summary on evidence-based wound care practices is worth keeping in your reading stack.
Then ask what the product actually does
Many notes get lazy. For instance, “Applied foam dressing” says almost nothing. The better question is whether the product donates moisture, gels with exudate, wicks vertically, protects the periwound, supports autolytic debridement, or fills undermining without packing too tightly.
If you can't state the function in one sentence, you probably haven't justified the choice.
Don't ignore patient and practice realities
The best dressing on paper fails if the patient can't keep it in place, can't afford the supply pattern, or needs a simpler change schedule because caregiver support is unreliable. “What is available” and “what is practical” aren't afterthoughts. They're part of the clinical decision.
Use this quick framework in order:
- Wound need: moisture, absorption, protection, fill, debridement support, or infection control.
- Product function: what the dressing class contributes.
- Patient factors: pain, tolerance, mobility, adherence, psychosocial barriers.
- Operational fit: formulary, home supply access, change frequency, clinician time.
- Documentation defense: one sentence linking wound findings to dressing purpose.
Good dressing selection is usually less about finding the perfect product and more about choosing the most appropriate function you can defend.
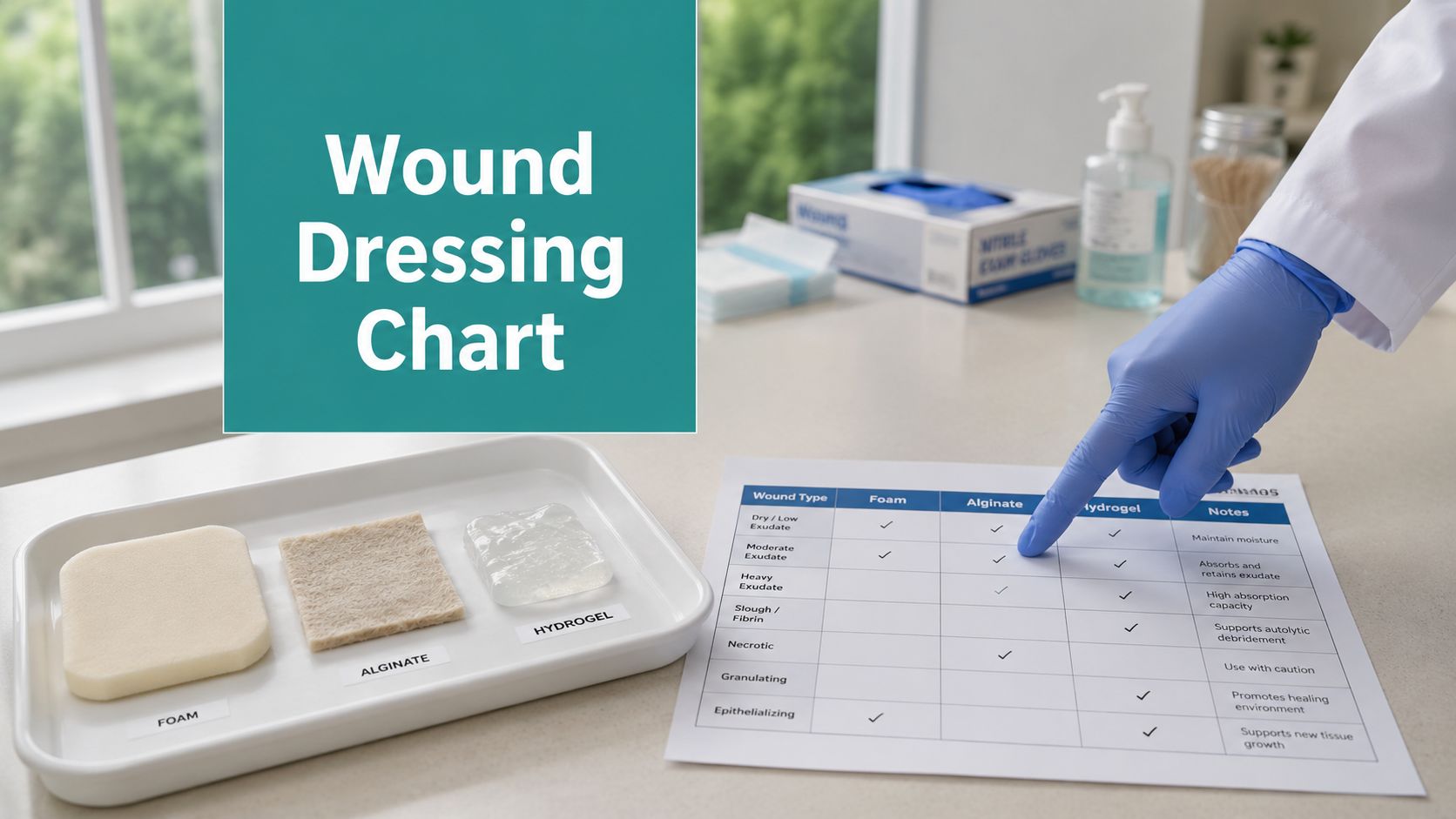
The Wound Dressing Selection Chart
Use the chart below as a starting point, not a rigid rule. Before choosing anything, document the wound assessment. The minimum useful assessment includes exudate characteristics and amount, wound bed tissue, wound edge characteristics, and periwound condition, as specified in the CLWK wound dressing selection guideline.
Read the first column for the dominant wound feature. Then match it to the primary goal. That gives you a reasonable first-line dressing class and one alternative if supply, tolerance, or wear time makes the first choice less practical.
Wound Dressing Selection Chart by Wound Characteristics
| Wound Characteristic | Primary Goal | First-Line Dressing Class | Second-Line / Alternative | Clinical Note |
|---|---|---|---|---|
| Dry wound bed, scant exudate | Add moisture | Hydrogel | Low-adherence contact layer with secondary cover | Avoid drying the wound further with overly absorptive products |
| Granulating wound, light to moderate exudate | Protect and absorb | Foam | Silicone foam | Good for fragile tissue when you need atraumatic removal |
| Sloughy wound with moisture present | Support autolytic debridement | Hydrocolloid | Hydrogel with absorptive secondary dressing | Don't use an occlusive approach if infection is suspected |
| Copious exudate | Absorb and protect periwound | Alginate | High-absorption foam | Reassess frequently for strike-through and maceration |
| Tunneled or undermined wound | Fill dead space appropriately | Alginate rope | Hydrogel-based filler with secondary cover | Fill the space without overpacking |
| Fragile periwound, shear-prone location | Minimize trauma | Silicone foam | Non-adherent contact layer with secondary absorbent cover | Useful on mobile areas and newly epithelializing wounds |
| Stable dry eschar | Keep dry and protected | Dry protective cover | Film only if appropriate to surrounding skin and goal | Don't add moisture if the plan is to maintain dry stability |
| Malodorous wound or signs concerning for local infection | Manage bioburden | Antimicrobial dressing | Standard absorptive dressing after reassessment if infection resolves | Don't let antimicrobial use continue without a review point |
How to use it well
The chart works only when your assessment is current. If exudate drops from copious to moderate, or if epithelialization begins, the dressing should often become less aggressive. If odor appears, or the periwound turns erythematous, you may need a different approach entirely.
That's why a wound dressing selection chart belongs beside your assessment process, not in place of it.
Dressing Categories A Clinician's Breakdown
Dressing categories make sense when you think in functions. They become messy when people treat them like interchangeable shelf items. They aren't.
For day-to-day clinic work, I reduce the main categories to what they're good at, what they're bad at, and how to justify them in the note. If you want a parallel review of common wound healing dressings, keep that nearby. Then build your documentation around the wound findings.
Foams
Foams are your workhorse when you need absorption plus cushioning and periwound protection. They're often a good fit for moderate drainage, superficial depth, and wounds that need a gentle cover rather than active moisture donation.
What doesn't work is using foam as a reflex for every draining wound. A shallow, moderately draining wound can do well with foam. A deep cavity with dead space won't.
Documentation pearl: Document the exudate level, the periwound risk, and the goal. Example: “Moderate serosanguineous drainage with intact but fragile periwound. Foam selected for absorption and protection of adjacent skin.”
Alginates
Alginates earn their place when exudate is heavy or when you need a conforming filler for depth, undermining, or tunneling. They're useful because they manage fluid while helping the wound avoid pooling.
Where clinicians get in trouble is stuffing them into a tunnel too tightly or leaving them in place after the exudate profile has clearly changed.
Documentation pearl: State both drainage burden and depth. “Copious drainage with tunnel present. Alginate rope used to fill dead space lightly and manage exudate.”
Hydrogels
Hydrogels are for wounds that need moisture. They can support autolytic debridement and are often helpful when tissue is dry, slough is adherent, or removal trauma is a concern.
They fail when used on wet wounds that already have too much fluid. Then you're feeding maceration.
Documentation pearl: Tie the product to wound-bed dryness. “Dry wound bed with adherent nonviable tissue. Hydrogel selected to donate moisture and support autolytic debridement.”
Hydrocolloids
Hydrocolloids still have a place, especially where you want occlusion and support for autolysis in a properly selected wound. But they're not harmless default covers. Using them on a wound with suspected infection is a common mistake.
If the wound is sending infection signals, don't trap that problem under an occlusive plan and hope the note will save you later.
Documentation pearl: Explain why an occlusive strategy fits. “Lightly draining sloughy wound without signs of spreading infection. Hydrocolloid chosen to maintain moisture balance and support autolytic debridement.”
Transparent films and contact layers
Films and non-adherent contact layers are about protection, visibility, and low trauma. They're often useful over shallow wounds, fragile skin, or as part of a layered approach where the secondary dressing handles fluid.
They don't solve absorption problems. If the wound is wet, film alone is usually the wrong answer.
Documentation pearl: Describe the protection need. “Fragile periwound and epithelializing wound edge. Non-adherent contact layer applied to minimize trauma during dressing changes.”
Antimicrobial dressings
These are not a lifestyle. They're a targeted intervention for wounds with local infection concerns or increased bioburden. If the only reason the wound is still on an antimicrobial after multiple visits is “that's what we started with,” you're drifting.
Documentation pearl: Record the infection indicators you observed and your review plan. “Local signs concerning for infection noted. Antimicrobial dressing initiated with planned reassessment at follow-up.”
Managing Infection and Bioburden with Dressings
You see the patient on Tuesday. The wound looked stalled last week, and now the drainage has increased, the odor is still present after cleansing, and the periwound is starting to look angry. No fever. No obvious systemic decline. This is the visit where clinicians either make a focused antimicrobial plan or drift into another week of vague charting and a dressing choice they cannot defend later.

The practical rule is simple. Use antimicrobial dressings as a time-limited treatment trial, not a standing habit. A common approach is a 2-week review window, which aligns with published wound dressing guidance on reassessing antimicrobial use and stopping it once the indication is gone, as outlined in this dressing selection guidance.
That review point matters for two reasons. First, the wound should declare itself by then. Second, payers want to see why you started an antimicrobial and why you continued it.
What should trigger the switch
Do not wait for cellulitis or systemic illness before questioning the plan. Local deterioration is enough to reassess. Persistent odor after cleansing, increased exudate, new friability, worsening periwound erythema, increased pain, or a wound bed that keeps producing slough despite otherwise appropriate care all support a closer look at infection burden or biofilm.
If the wound improves in one area but worsens in another, count that as mixed response, not success. Less visible slough does not outweigh rising drainage and odor.
For wounds that keep stalling despite reasonable moisture balance and debridement, persistent surface contamination is often part of the story. This overview of biofilm on skin and chronic wound behavior is useful background if you want a quick refresher on why some wounds look only mildly inflamed but still refuse to progress.
What the note should say
Newer clinicians lose ground with payers. “Continue antimicrobial dressing” is not a defensible note by itself. The chart has to show the observed problem, the reason a standard moisture-management dressing was no longer enough, and the planned stop or switch date.
Document these points clearly:
- Clinical indicators present: odor after cleansing, change in exudate character or volume, erythema, pain, edema, friable tissue, delayed healing trajectory
- Why you chose an antimicrobial dressing: concern for local infection, increased bioburden, or recurrent stall despite appropriate basic wound management
- What you will reassess: drainage, odor, tissue quality, periwound condition, wound measurements, and patient symptoms
- When you will change course: explicit follow-up interval and what would justify discontinuing, continuing, or switching the dressing
A note that works in actual settings sounds like this: “Wound demonstrates persistent odor after cleansing, increased seropurulent drainage, friable granulation tissue, and worsening periwound erythema compared with prior visit. Findings raise concern for local infection or increased bioburden. Antimicrobial dressing initiated today with reassessment planned in 14 days or sooner if erythema extends, pain increases, or drainage escalates.”
That level of detail does two jobs. It guides the next visit, and it shows the antimicrobial was chosen for active clinical findings rather than routine habit.
One more point. Dressing failure in an infected or high-bioburden wound is often subtle before it becomes obvious. The wound gets wetter at the edges. The tissue bleeds a little more during cleansing. The patient reports more tenderness, but the measurements barely change. Those are the cases where disciplined reassessment saves time, reduces avoidable product cycling, and gives you documentation you can defend if reimbursement is questioned later.
Solutions for Deep Wounds and Difficult Locations
Flat wounds are easy. The problems start when depth, motion, contour, and moisture all work against you.
A tunneled wound isn't just a deeper shallow wound. A dressing for a heel doesn't behave the same way on a sacrum or over a knee. If you don't plan for dead space, shear, and dislodgement, the dressing fails even if the category was technically correct.
Fill dead space without creating pressure
The distinction that matters is filling versus packing. You want contact with the wound surface and management of dead space. You do not want a tightly packed cavity that creates pressure, impairs drainage, or traumatizes tissue at removal.
For a tunneled or undermined wound, choose a filler that conforms and can be removed completely. If the wound is dry, moisture support may matter more. If it's draining heavily, the filler has to manage fluid instead of just occupying space.
Use a quick mental check:
- Dry depth: choose a moisture-supportive filler strategy.
- Wet depth: choose an absorptive filler strategy.
- Fragile tunnel tissue: choose the least traumatic removal option that still manages the wound environment.
Match the dressing to the body site
Mobile joints, digits, heels, and sacral contours all challenge fixation. The best product on the shelf won't help if it lifts at the edges or channels exudate laterally into the periwound.
For awkward locations:
- Knees and other joints: prioritize flexibility and secure fixation.
- Heels: think offloading first, then choose a cover that won't bunch or slip.
- Sacral area: expect moisture, friction, and lift. Protect surrounding skin aggressively.
- Digits: bulk becomes a problem fast. Keep the dressing functional and compact.
For surgical wounds, this issue gets even more specific. Dressings that support undisturbed wound healing with wear times of up to 7 days matter because changing them too often disrupts the healing environment. They should be changed only for absolute indicators such as saturation, excessive bleeding, or suspected infection, based on the Wounds International consensus on incision care.
Protect the periwound like it matters
It does. A good dressing plan can fail because the surrounding skin breaks down first. Venous ulcers are a classic example. If the periwound is already excoriated or macerated, choose a dressing that handles exudate without spreading it sideways and stripping the skin at each change.
This is also where a lot of newer clinicians under-document. “Periwound intact” is not enough if it's fragile, wet, erythematous, or indurated. The surrounding skin often explains why the dressing you chose was medically necessary.
Documentation and Coding That Justifies Your Choice
A clinician can make the right dressing decision and still lose the reimbursement argument. That usually happens because the note names the product class but never links it to the wound findings. Payers don't cover dressings because they sound advanced. They cover them when the chart shows medical necessity.
The reimbursement standard is practical. Cost-effectiveness includes indirect costs like dressing change frequency, not just unit price, and the clinician should document why a specific dressing was chosen based on formulary availability and the wound's needs, such as autolytic debridement support or high exudate management, as described in the WoundSource review of dressing selection basics.
What a defensible note includes
Your wound note should make a reviewer's job easy. That means documenting the assessment in a way that naturally leads to the dressing choice.
At minimum, chart:
- Wound measurements and depth: include tunneling or undermining when present.
- Tissue description: granulation, slough, eschar, exposed structures if applicable.
- Exudate profile: type and amount.
- Edge and periwound findings: attached, rolled, excoriated, indurated, erythematous, macerated.
- Clinical rationale: why this dressing class fits this wound now.
- Change frequency: especially if it differs from a simpler option.
- Supply or formulary context: when it affected your choice.
A good one-line rationale sounds like this: “Moderate serosanguineous drainage with fragile periwound and shallow depth. Silicone foam continued for absorption, low-trauma removal, and protection of surrounding skin.”
Where coding and dressing choice meet
If you debride, the dressing rationale should still follow the post-procedure wound bed. For debridement CPT codes 11042–11047, the post-debridement note should describe what tissue was removed, the resulting wound characteristics, and why the selected dressing supports the new wound state. If you just performed sharp debridement and then chart a generic “dry sterile dressing applied,” you've missed a chance to support medical necessity for the actual supply strategy.
Surveyors and payers look for consistency between the procedure, the wound description, and the treatment plan. They also notice when clinicians keep ordering specialty dressings without documenting why gauze or a simpler cover wouldn't meet the need.
Common denial triggers
Documentation mistake: Expensive dressing ordered, no explicit statement of what problem it solves better than a basic alternative.
Three frequent problems show up over and over:
- Assessment-documentation mismatch: the wound is described as dry, but the plan uses a highly absorptive dressing with no explanation.
- No justification for specialty supply use: the note names the dressing but not the functional reason.
- Weak continuity: the wound changed, but the treatment rationale didn't.
If your team still manages payer forms manually, even small errors in supply requests and prior auth paperwork can slow things down. A simple online tool for PDF forms can help staff complete documentation packets cleanly before submission, especially when wound supply vendors or payers still require static forms.
Common Scenarios and Pitfalls in Practice
A patient returns for follow-up, the wound looks a little better, and the original dressing order stays in place because no one wants to disrupt progress. That is one of the easiest ways to drift into poor wound care and weak documentation at the same time. A dressing chart helps at the bedside, but in practice the harder job is knowing when the wound has changed just enough to justify a different product, a different frequency, or a different level of supply.
Wagner Grade 2 diabetic foot ulcer with falling exudate
At the first visit, heavier drainage may support an absorptive filler or a higher-fluid-handling secondary dressing. Two visits later, exudate has dropped, the base is cleaner, and a thin rim of epithelialization is present. That is usually the point to step down. A softer protective option, often a silicone foam or another low-trauma cover, makes more sense than continuing a dressing chosen for a wetter wound.
The common mistake is leaving the original order untouched because the wound is improving. Improvement is the reason to change the plan.
Document the clinical cue and the operational reason. A defensible note sounds like this: "Exudate decreased from moderate to scant. Fragile new epithelial tissue at wound edge. Dressing changed to lower-trauma protective category to control light drainage and reduce disruption during removal." That gives the next clinician a rationale and gives the payer a reason the supply changed.
Venous ulcer with macerated periwound
A venous leg ulcer can have a wound bed that looks acceptable while the surrounding skin is failing. In clinic, that matters just as much as the center of the wound. If the periwound is white, boggy, or starting to break down, the current dressing is not managing moisture well enough, even if the wound dimensions are stable.
The pitfall is charting only length, width, depth, and drainage amount, then renewing the same foam without addressing where the fluid is going. Lateral spread is still fluid mismanagement. The note should describe the periwound condition, the drainage pattern, and what was added or changed to protect intact skin. If you use a barrier product, a different cover dressing, or a more absorptive layer, say why. That is often the difference between a note that supports medical necessity and one that reads like autopilot care.
Stable heel eschar
A dry, adherent heel eschar calls for restraint. If there is no drainage, no fluctuance, no erythema extending into surrounding tissue, and no other sign that the eschar has become unstable, the goal is protection, pressure control, and close observation.
The mistake is adding moisture because the wound looks dry. On a stable heel, that can create problems you did not have at the last visit. Chart stability clearly. "Dry, firm, adherent eschar remains intact. No drainage or edge lifting. Protective dry cover continued with offloading." That is a stronger plan than vague wording about routine dressing care.
One more pattern shows up often in busy clinics. Subtle decline gets missed because the wound has not changed enough to trigger alarm. A little more odor. Drainage that turns thicker. Periwound erythema that was absent last week. Increased pain during cleansing in a patient who usually reports none. Those are the moments to reconsider the category, not just reorder what is already on the supply sheet. If you switch because the wound trajectory changed, say that plainly in the note.
If your team is spending too much time turning solid clinical decisions into billable documentation, EkagraHealth AI is worth a close look. It's built for wound care practices that need faster SOAP notes, cleaner CPT and ICD-10-CM mapping, and fewer missed details between the bedside and the claim.
