CPT 99213 is the workhorse code for an established patient office or outpatient follow-up visit that takes 20 to 29 minutes on the date of service or meets low-complexity medical decision making. In wound care, that usually means a routine recheck of a stable chronic wound where the plan stays straightforward, the risk stays low, and the chart clearly shows why the wound is stable.
You know the visit. Diabetic foot ulcer follow-up. Dressing tolerated. Offloading reviewed. Wagner grade unchanged. Minimal exudate. No new odor, no new undermining, no spreading erythema, no change in systemic status. The patient needs assessment, reinforcement, and a real note. They do not need a level inflated beyond the work performed.
That's where people get 99213 wrong in both directions. Some clinics overreach and turn every wound follow-up into 99214. Others default to 99213 so often that they leave money on the table when debridement, infection risk, or data review clearly push the visit higher. The bigger issue now is that “routine follow-up” no longer carries much weight by itself. If you want 99213 to stand up, your note has to show wound stability in clinical terms, not just in billing language.
The Daily Workhorse Code for Wound Care Follow-Ups
A stable Wagner grade 1 diabetic foot ulcer is the classic 99213 visit. The patient returns, the wound bed is clean, drainage is still scant and serous, the periwound skin is intact, and the offloading plan hasn't changed. You review the interval history, inspect the ulcer, confirm there's no dehiscence, reinforce dressing instructions, and set the next follow-up.
That encounter is exactly why 99213 exists. It is a Level 3 E/M service for an established patient in the office or outpatient setting, used when the work supports low-complexity MDM or the total time supports the code. In wound care, that means the visit is still medically necessary, but the problem addressed is stable and the management is not escalating.
What this looks like in real clinic flow
The code fits best when the wound is chronic but not actively worsening. Think:
- Stable diabetic foot ulcer: Wagner grade unchanged, minimal exudate, no new necrosis, no new tunnel or sinus tract.
- Slowly improving venous leg ulcer: edema is being managed, drainage pattern is familiar, dressing plan remains the same.
- Pressure injury follow-up: no major change in depth or tissue type, no new signs that would change treatment risk.
Practical rule: If your assessment reads like “unchanged, low risk, limited review, continue current plan,” you're usually in 99213 territory.
The mistake is treating 99213 like a generic default. It isn't. It's a specific code for a specific level of work. In wound care, that means your note should match the clinical reality, not the billing habit.
Justifying 99213 Using Time or Medical Decision Making
There are two valid ways to support 99213. You can bill it by total time or by medical decision making. CPT 99213 is a Level 3 evaluation and management service for an established patient office or outpatient visit, requiring either low-complexity medical decision-making or a total encounter time of 20 to 29 minutes on the date of service. In wound care, it fits routine follow-ups of stable chronic wounds, such as a Wagner grade 1 diabetic foot ulcer with minimal exudate and no dehiscence, where the provider reviews limited data, addresses a single diagnosis, and uses straightforward treatment with low risk, as outlined in this 99213 wound care coding reference.
The time pathway
If you're billing by time, count the total professional time on the date of service, not just the face-to-face portion. In a wound clinic, that often includes chart review, reviewing a recent lab, evaluating the wound in person, counseling on dressing changes or offloading, documenting the note, and ordering a basic follow-up item if needed.
That's where many clinicians get sloppy. They do the work, but they don't state the time. If time is your basis, document it plainly.
Examples of time that can count on the date of service:
- Pre-visit review: prior wound photos, last visit note, recent CBC or culture result if relevant and limited.
- Face-to-face evaluation: wound inspection, periwound assessment, patient education, treatment discussion.
- Post-visit work: note completion, simple order entry, coordination related to the encounter.
If your team needs a clean way to think about what counts as professional time, this short explanation of billable hours explained is useful as a general framework, even though medical coding has its own rules. For therapy-style timed services, this separate issue matters too, and the distinction is different from E/M coding under the Medicare 8-minute rule.
The MDM pathway
Low MDM in wound care usually means the problem is stable, the data review is limited, and the management risk remains low. A single stable chronic wound often fits. A stable Wagner grade 1 DFU with no new infection concern is a common example.
The core questions are practical:
Problems addressed
Are you managing one stable chronic illness, or something minor and uncomplicated?Data reviewed
Did you review limited information, such as a recent lab or prior note, without getting into extensive new workup?Risk
Did the treatment plan remain straightforward and low risk, without a major therapeutic escalation?
If the wound is stable but the treatment risk or data review escalates, the code may no longer be 99213.
A note that says only “follow-up wound care, continue same dressing” is weak. A note that states wound status, tissue quality, exudate type, periwound condition, and why the plan remains unchanged is much stronger.
Applying MDM and Time Rules in a Wound Clinic
In real clinic work, abstract coding language becomes concrete fast. “Low complexity” isn't a theory problem. It's whether the wound, the review, and the treatment risk stayed limited enough to justify a Level 3 visit.
The projected 2026 national average reimbursement for CPT 99213 is approximately $91.46, and it's described as roughly 70% of the reimbursement for 99214. That's why the distinction matters operationally, not just academically. The same source also notes that the code is valid for face-to-face and telehealth visits as long as the time or MDM criteria are met, which makes the documentation standard, not the visit format, the deciding factor in many cases. See this analysis of 99213 and 99214 reimbursement and coding differences.
What low complexity looks like at the bedside
A venous leg ulcer follow-up can still be 99213 if the visit stays clinically restrained. Compression is working. Edema is controlled. Drainage is light serous. The ulcer is still present, but there's no new cellulitis, no abrupt increase in slough, and no need to change the overall care path.
A diabetic foot ulcer check can also fit if the chart supports stability. You inspected the wound, verified no new dehiscence, confirmed offloading adherence, reviewed a limited item from the chart, and continued the same treatment plan.
Typical low-complexity wound elements include:
- Problem profile: one stable chronic wound, not actively deteriorating
- Data: limited review, not an extensive diagnostic workup
- Risk: straightforward treatment, no meaningful escalation in management risk
What counts toward the 20 to 29 minutes
In a wound clinic, the time-based path often makes sense when the visit is more labor-intensive than the MDM looks on paper. Teaching alone can take time, especially with dressing technique, pressure redistribution, edema control, or offloading reinforcement.
Here's the kind of work that often fills the clock legitimately:
- Chart review before entering the room: prior measurements, previous treatment response, recent lab trend already in the chart
- Direct patient work: history update, wound inspection, periwound assessment, counseling on dressing changes, adherence barriers, moisture balance
- Documentation after the encounter: wound measurements, exudate description, tissue findings, plan, follow-up instructions
A stable wound can still justify 99213 by time if the note clearly ties the total professional time to same-day work.
What doesn't work
What fails is vague shorthand. “Routine recheck.” “Stable.” “No change.” That language tells a payer almost nothing.
For wound care, the better note names the wound trajectory in concrete terms: exudate remains minimal, Wagner grade unchanged, periwound maceration absent or improved, and dressing plan maintained because the wound is clinically stable. That's what makes the chart believable.
Defensible Documentation Snippets for 99213
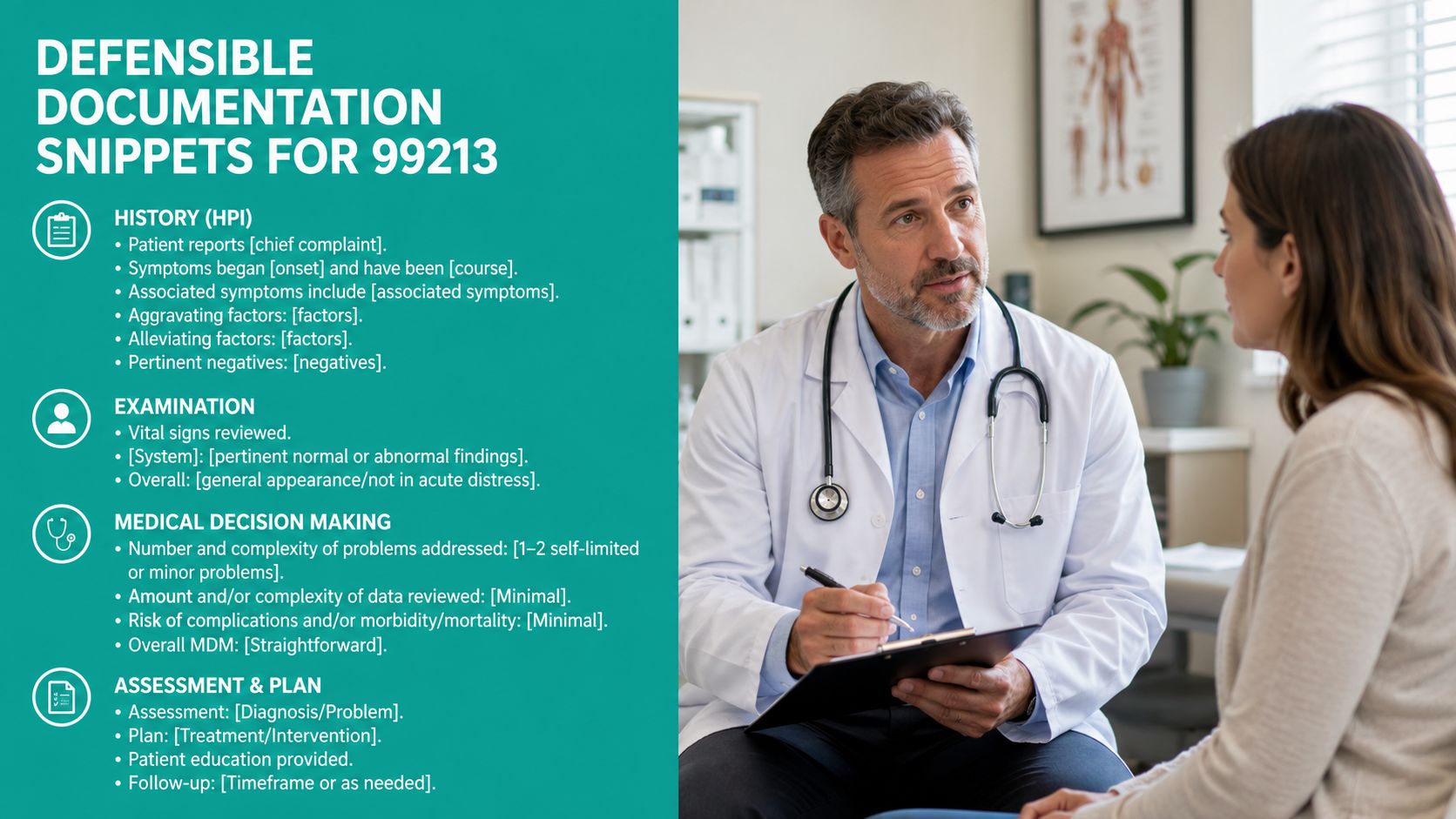
CPT 99213 applies when the patient has a single stable chronic condition, such as a non-healing wound on a stable care plan, with minimal data review and low risk. The chart must support either an expanded problem-focused history and exam or low-level MDM, and audits often catch practices that blur the line with 99214. This 99213 documentation overview for established patient follow-ups gets the core point right: the code is built for visits where wound status is stable, Wagner grade hasn't changed, and exudate remains minimal.
Snippet for a stable Wagner grade 1 diabetic foot ulcer
Use wording that shows why the wound is stable, not just that you saw it.
Assessment
Established patient seen for follow-up of chronic diabetic foot ulcer, Wagner grade 1. Ulcer remains stable on current care plan. No dehiscence, no malodor, and no increase in drainage. Exudate minimal and serous. Periwound skin intact without new maceration or spreading erythema. No new tunneling or undermining appreciated.Plan
Continue current dressing regimen and offloading. Reinforced pressure avoidance and return precautions. Low-complexity follow-up management appropriate based on stable chronic wound and low-risk treatment plan.
Snippet for a pressure ulcer with minimal serous drainage
A pressure injury follow-up often gets under-described. Include tissue status and periwound findings.
- History: Patient returns for established follow-up. Reports dressing adherence and no new pain, fever, or increased drainage.
- Exam: Pressure ulcer evaluated. Wound bed without significant interval deterioration. Drainage minimal, serous. Periwound skin without new excoriation or significant maceration. No new odor or signs of acute soft tissue spread.
- Plan: Continue current local wound care and pressure redistribution measures. No change in overall management risk today.
Snippet for a venous leg ulcer that is improving slowly
“Stable” can be too blunt. If it's slowly improving, say that.
Venous leg ulcer follow-up in established patient. Wound continues gradual improvement on current treatment plan. Drainage remains light and serous. Periwound skin shows no new breakdown. Edema control reviewed and current compression strategy reinforced. No findings today suggesting escalation in risk or need for more complex decision making.
Snippet for billing by time
If time supports the code, document it explicitly.
Total time spent on date of service: 25 minutes. Time included review of prior wound documentation, face-to-face interval history and wound assessment, counseling on dressing change technique and offloading adherence, and completion of encounter documentation and treatment plan.
That single sentence is often the difference between a defendable claim and a weak one.
Practical note construction
Many clinicians dictate details faster than they type them, especially during busy follow-up blocks. If your process relies on spoken notes, understanding how speech becomes text helps reduce omissions and cleanup time. This plain-language piece on understanding AI audio to text conversion is a useful primer. For wound-specific charting structure, a focused wound care documentation template is more useful than a generic follow-up template because it prompts the details payers require.
Don't clone last week's note and change one adjective. Stable doesn't mean identical. Every visit still needs a current wound story.
The Costly Mistake of Undercoding with 99213
A lot of wound clinics have the opposite problem from what auditors usually warn about. They don't overcode every stable follow-up. They undercode the harder visits because 99213 feels safe.
That safety is expensive. The gap is in visits involving Wagner grade 2 to 3 wounds, obvious exudate, and debridement, where the work may support 99214 because the MDM rises to moderate through data review or treatment risk. A 2025 RCM audit found 99213 billing persisted in 68% of such cases, with an estimated loss of $12 to $18 per visit. That undercoding pattern is summarized in this wound care review of 99213 underuse and 99214 opportunities.
When debridement changes the level
Doing debridement doesn't automatically make the E/M higher. But pretending the encounter is still low complexity when the wound has obvious worsening features is where clinics miss the mark.
If you're evaluating a wound with purulent drainage, reviewing new labs or imaging, deciding whether infection burden has changed, and selecting procedural management such as 11042 to 11047 based on tissue depth and wound characteristics, the visit may no longer fit the low-risk, limited-data profile of 99213.
Common scenarios that push away from 99213:
- Wagner grade 2 or 3 wound: especially if there's notable tissue involvement beyond a superficial stable ulcer
- Obvious exudate shift: serous to purulent, or a clinically significant increase in drainage burden
- Debridement decision-making: selecting among 11042 to 11047 because tissue depth and risk matter
- Additional data review: labs, imaging, or external records that meaningfully affect treatment
The mistake isn't performing debridement and billing an E/M. The mistake is ignoring how the wound's complexity changed the MDM.
CPT 99213 vs 99214 at a Glance
| Criteria | CPT 99213 (Level 3) | CPT 99214 (Level 4) |
|---|---|---|
| Patient type | Established patient | Established patient |
| Time | 20 to 29 minutes | 30 to 39 minutes |
| MDM | Low complexity | Moderate complexity |
| Typical wound scenario | Stable chronic wound follow-up with minimal exudate and low risk | Wound follow-up with greater treatment risk, more involved data review, or more complex management |
| Wound status | Stable, limited change | More clinically involved, often with factors that increase risk or management intensity |
| Debridement context | May still fit if E/M work remains low complexity and separately supported | More likely when debridement decision reflects moderate MDM due to wound severity, data, or risk |
What works better than a coding habit
Stop asking whether a visit “felt like a routine follow-up.” Ask what the note supports.
A stable wound check with minimal exudate and no treatment escalation belongs in 99213. A more involved visit with meaningful risk assessment, deeper tissue management, or new diagnostic review may deserve 99214. The code should follow the work. Not the clinic's comfort level.
Modifiers and Payer Rules to Prevent Denials

A clean 99213 claim needs more than the right code. It needs a note that shows why the visit stands on its own, and it needs claim details that match the encounter.
The denial trend that matters most in wound care right now is documentation vagueness. A 2025 CMS Bulletin found 41% of 99213 denials in wound care were tied to vague “routine follow-up” statements lacking wound trajectory data, including healing progress and exudate change. The same source says clinicians now need to document Wagner grade stability, debridement necessity, and dressing change rationale to avoid preventable receivable delays. See the summary in this CMS-focused discussion of 99213 denial patterns in wound care.
Modifier 25 has to be earned
If you perform a procedure on the same date, such as debridement, and also bill an E/M, the E/M must be significant and separately identifiable. That standard is stricter than many notes suggest.
What supports modifier 25 in wound care:
- Separate evaluation work: interval history, wound reassessment, decision-making beyond the procedural note
- Distinct medical necessity: management of the wound condition itself, not just the technical performance of debridement
- Clear documentation split: procedure note and E/M assessment should read like separate services, not one duplicated paragraph
For a practical coding breakdown, this review of Modifier 25 in CPT billing is worth keeping handy.
Payer-facing details that often break the claim
Place of service matters. So does wording. So does whether your note gives the payer a trajectory instead of a label.
What surveyors and auditors tend to look for in a wound follow-up note:
- Wound stability described clinically: Wagner grade unchanged, exudate pattern stable, no new dehiscence
- Periwound assessment: maceration, erythema, edema, callus, or other surrounding skin findings
- Reason current treatment continues: dressing choice, offloading, edema control, or pressure redistribution rationale
- Procedure necessity if done: why debridement was needed that day, not just that it occurred
“Routine follow-up” is scheduling language. It is not wound documentation.
If your note tells the wound story in concrete terms, denials drop. If it reads like a calendar entry, payers will treat it that way.
Final Check for a Defensible 99213 Note
Before choosing 99213, make four checks. Confirm the wound visit really stayed low complexity. Make sure the chart shows wound stability in concrete clinical language. If billing by time, state the total time clearly. If a procedure happened the same day, separate the E/M work from the procedure work.
Then verify the foundation. 99213 is only for an established patient, and that means the patient must have received professional services from a physician of the same specialty in the same group practice within the past three years, as described in this established patient rule for CPT 99213. Miss that requirement and you're in new-patient code territory, regardless of how straightforward the wound follow-up was.
If your team is tired of chasing missing wound details, fixing cloned follow-up notes, and sorting out E/M levels after clinic ends, EkagraHealth AI is built for that exact workflow. It helps wound care practices capture the wound story during the visit, draft stronger documentation, support CPT and ICD-10 coding, and get cleaner claims out the door without adding more charting to the end of the day.
