Evidence-based wound care isn’t just a buzzword; it’s a fundamental shift away from routine, ritual-based treatments toward a smarter, more effective strategy. It’s about methodically blending top-tier research with seasoned clinical expertise and, crucially, the patient’s own values and preferences. This philosophy ensures every decision, from the initial assessment to the final dressing choice, is intentional and supported by solid data.
The results of this approach are compelling: faster healing times, significantly lower infection rates, and far more efficient, cost-effective care. It has rightfully become the gold standard for a simple reason: it consistently delivers superior outcomes for patients while strengthening the operational health of the healthcare system. For any organization serious about improving patient care and managing resources wisely, mastering evidence-based wound care practices is no longer optional—it’s essential.
Why Evidence-Based Wound Care Is Now Standard Practice

Think of evidence-based wound care as a highly sophisticated GPS for healing. Not long ago, many clinicians relied heavily on tradition or anecdotal experience—the classic “this is how we’ve always done it” mindset. While well-intentioned, this approach led to a Wild West of inconsistent care, where patient outcomes could vary wildly from one facility to another, or even between clinicians working in the same building. This variability not only affected patient well-being but also created unpredictable costs and inefficiencies.
That inconsistency is precisely the problem evidence-based care was designed to solve. Instead of navigating with an old, hand-drawn map based on past journeys, clinicians now have a dynamic system that shows them the most direct and effective route to resolving a wound. It integrates real-time data, scientific evidence, and professional judgment to create a clear, reliable path forward.
This modern framework stands on three core pillars that guide every clinical decision, ensuring a holistic and patient-centered approach.
The Three Pillars of Modern Wound Care
At its heart, this isn’t a rigid, one-size-fits-all formula that stifles clinical judgment. It’s a balanced, dynamic strategy that requires a skillful blend of the best information available to create a treatment plan that’s both scientifically sound and deeply personal.
- The Best Research Evidence: This is the cornerstone. It means using findings from high-quality clinical studies—randomized controlled trials, systematic reviews, and meta-analyses—to inform what you do. It means choosing dressings, debridement methods, and adjunctive therapies because they have been scientifically proven to work for specific wound types and patient populations, not just because they’re familiar or heavily marketed.
- Clinical Expertise: A practitioner’s judgment, honed over years of hands-on experience, is irreplaceable. This pillar is what allows a clinician to take solid research and apply it intelligently to a specific patient’s unique and complex situation. It involves factoring in their overall health status, comorbidities, the wound’s specific characteristics, and the resources available in the care setting. Expertise turns science into a practical art.
- Patient Values and Preferences: The patient isn’t a passive recipient of care; they are an active partner in the healing process. Their personal goals, cultural beliefs, lifestyle, and financial constraints have to be part of the conversation. A treatment plan that is scientifically perfect but unmanageable for the patient is destined to fail. Incorporating patient preferences ensures better adherence, satisfaction, and ultimately, better outcomes.
By weaving these three elements together, evidence-based practice moves far beyond generic, impersonal protocols. It creates a personalized, evidence-informed roadmap for each patient, ensuring the chosen path is supported by science, guided by professional insight, and aligned with what the patient truly wants and needs.
This structured methodology is our best weapon against the staggering clinical and financial costs of outdated care. Chronic wounds affect about 8 million people globally, and the data paints a stark picture of the challenges. Studies show a clear link between infection control and healing, with 59% of chronic wounds healing when no infection is present.
But that number plummets to just 45% when infections are confirmed or even suspected. That’s a 14% drop in healing rates that directly translates to higher costs from longer treatments, more complex interventions, and extended hospital stays. You can learn more about how pathways optimize infection management.
By establishing a clear, data-driven standard of care, these practices pave the way for measurably reduced infection rates, faster healing trajectories, and better resource utilization across the board.
Applying the TIME Framework for Wound Bed Preparation
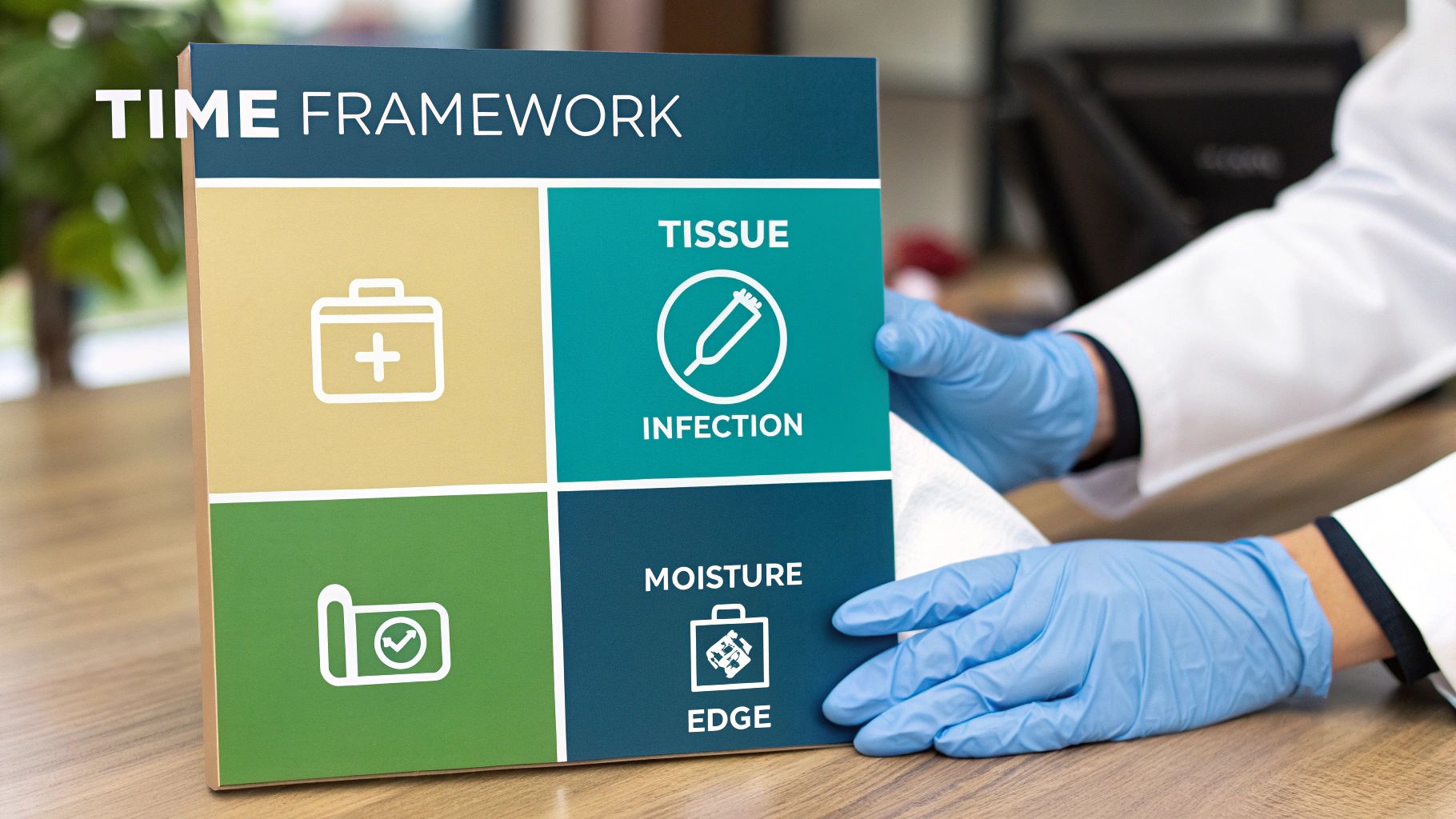
To make evidence-based wound care a consistent reality at the bedside, clinicians need a reliable, systematic way to assess a wound and prepare it for healing. That’s exactly what the TIME framework delivers. It’s more than just a handy acronym; it’s a structured, logical, and globally recognized process that takes the guesswork out of wound bed preparation and ensures all critical factors are addressed.
The TIME framework walks clinicians through four crucial components: Tissue, Infection/Inflammation, Moisture, and Edge. By methodically addressing each component in turn, you systematically remove the common barriers to healing and create the ideal environment for the body’s natural repair processes to take over.
Think of it like a skilled gardener trying to bring a neglected patch of soil back to life. You wouldn’t just scatter seeds and hope for the best. First, you’d meticulously pull the weeds (debridement), check for pests and diseases (infection control), ensure the soil has just the right amount of water (moisture balance), and prepare the edges of the plot to sustain new growth (edge advancement). The TIME framework brings that same deliberate, step-by-step logic to clinical practice.
To see how this works in practice, let’s break down each element in detail.
T is for Tissue Management
The first order of business is always the state of the tissue in the wound bed. What do you see? Is it healthy, pink, beefy-red granulation tissue, or is it covered with non-viable tissue like slough (the stringy, yellowish, or tan substance) or eschar (the tough, leathery, black or brown covering)? This dead tissue is a major problem—it acts as a physical barrier, blocking new cell growth and providing a perfect breeding ground for bacteria.
Best practice demands that we remove it. This process is called debridement, and the goal is simple: create a clean, healthy wound bed that’s ready for healing. The right method depends on the wound type, the patient’s condition, and the clinical setting. It might mean a skilled clinician performing sharp debridement at the bedside, using enzymatic ointments that selectively dissolve the dead tissue over days, or leveraging other advanced methods.
I is for Infection and Inflammation Control
With the wound bed cleared of non-viable tissue, you can shift your focus to managing the bioburden. It’s crucial to understand that all chronic wounds have some level of bacteria. The clinical challenge is keeping that bacterial presence from escalating into a full-blown infection that halts the healing process. This requires a sharp clinical eye, because the signs of a localized infection often go beyond the classic signs of redness and purulent discharge.
You have to look for the more subtle, secondary clues:
- Increased pain: Is the patient suddenly reporting more discomfort for no clear reason?
- Stalled healing: The wound was making steady progress, but now it’s stuck or even deteriorating.
- Friable granulation tissue: The otherwise healthy-looking tissue bleeds at the slightest touch.
- Atypical odor: There’s a new or worsening smell coming from the wound after cleansing.
When excessive inflammation or localized infection is the primary barrier, the next step might involve using antimicrobial dressings or topical antiseptics. Systemic antibiotics should be reserved for cases of spreading or deep tissue infection, guided by clinical protocols to avoid contributing to antibiotic resistance.
M is for Moisture Balance
Wound healing is a bit like the story of Goldilocks—it requires a moisture level that’s “just right.” If a wound bed is too dry, healthy new cells can dehydrate, slow their migration, and die. Conversely, if it’s too wet, the surrounding skin (the periwound) can become waterlogged and weakened, a condition known as maceration, which enlarges the wound.
The art and science of moisture balance is all about picking the right tool for the job. Your goal is to select a dressing that either donates moisture to a dry wound bed (like a hydrogel) or effectively absorbs excess fluid from a heavily draining one (like a superabsorbent polymer, foam, or alginate). The right choice creates that perfectly humid, balanced environment where cells can thrive.
Getting this right is absolutely critical. An inappropriate dressing choice can easily stall the healing process or cause further damage.
E is for Edge of Wound Advancement
Finally, turn your attention to the edges of the wound. Are they migrating inward, with new epithelial cells marching across the wound bed to close the defect? Or are the edges stalled—perhaps rolled under (epibole), thickened, and showing no signs of movement? When the edges aren’t advancing, healing has hit a definitive wall. To get a better handle on this, check out this helpful visual guide for accurate pressure injury staging.
If the edges are stuck, it’s a clear signal that an intervention is needed. You might need to debride the wound margins to stimulate new growth, consider advanced therapies like cellular and/or tissue-based products, or apply specific treatments that kickstart cellular activity. Focusing on the edge is how you guide a wound across the finish line to full closure.
This entire framework provides a comprehensive, repeatable strategy for every wound you encounter.
The TIME Framework At A Glance
This table summarizes the core goals and evidence-based interventions for each component of the TIME framework.
| Component | Clinical Goal | Evidence-Based Interventions |
|---|---|---|
| T – Tissue | Remove non-viable or deficient tissue to create a healthy, viable wound bed. | Sharp, enzymatic, autolytic, or mechanical debridement. |
| I – Infection/Inflammation | Identify and control infection and manage excessive inflammation. | Topical antimicrobial dressings, systemic antibiotics (if warranted), anti-inflammatory agents. |
| M – Moisture | Achieve a balanced moisture level to support healing and prevent maceration. | Selecting appropriate dressings (e.g., hydrogels for dry wounds, foams/alginates for wet wounds). |
| E – Edge | Stimulate epithelial migration from the wound edges for complete closure. | Debridement of non-advancing edges, advanced therapies (e.g., growth factors, skin substitutes), proper offloading and compression. |
By consistently applying this powerful framework, clinical teams can move from reactive, inconsistent care to a proactive, evidence-based approach that systematically supports and accelerates healing.
Choosing Interventions Backed By Clinical Evidence

You’ve performed a thorough assessment and have a clear picture of the wound’s status using a framework like TIME. Now what? This is where the rubber meets the road. It’s time to act on your findings, and this is the absolute core of evidence based wound care practices. Every choice must be deliberate and justified.
We’re moving beyond simply picking a product that’s readily available in the supply closet. Every single choice—from the type of debridement to the category of dressing—needs to be backed by solid clinical evidence showing why it is the appropriate intervention for this wound at this specific time. This critical-thinking mindset shifts wound care from a routine checklist into a precise, targeted strategy aimed at achieving complete and timely wound closure.
Evidence-Based Debridement Methods
Clearing out non-viable tissue is a critical first step. You simply must prepare the wound bed for healing. But how you do it matters immensely. Think of it like a delicate repair job: you wouldn’t use a sledgehammer on a fine watch. The debridement method has to be carefully matched to the wound characteristics, the patient’s condition, and the clinical setting.
- Sharp Debridement: This is the fastest, most direct approach for removing dead tissue. A trained clinician uses a scalpel, curette, or forceps to physically remove devitalized tissue. It’s the gold standard for thick, leathery eschar or when an urgent need exists to remove a source of infection.
- Enzymatic Debridement: This is a more targeted and selective method using a prescription ointment containing enzymes. These enzymes specifically break down and liquefy necrotic tissue while leaving healthy granulation tissue unharmed. It’s an excellent, less painful option for patients who cannot tolerate a sharp procedure or in settings where sharp debridement is not feasible.
- Autolytic Debridement: Here, we leverage the body’s own natural processes. By applying a moisture-retentive dressing, we create the perfect environment for the body’s own enzymes and phagocytic cells to dissolve dead tissue. It’s the most gentle and selective method, but it’s also the slowest.
- Mechanical Debridement: This involves the physical removal of debris. The old-school wet-to-dry dressing falls into this category, but modern evidence has shown it to be non-selective and capable of harming healthy tissue, which is why it has largely fallen out of favor. Newer options, like monofilament debridement pads, offer a much gentler and more effective alternative for surface debris.
Tackling Infection and Bioburden
Managing the bacterial load in a wound is a delicate balancing act. Current evidence strongly steers us away from the reflexive use of systemic antibiotics for non-systemic issues and points us toward more targeted, local treatments. The real clinical skill lies in matching the intervention to the level of bioburden.
For wounds with localized signs of infection, topical antiseptics or antimicrobial dressings are the first line of defense. A fantastic quality improvement project at Doncaster and Bassetlaw Teaching Hospitals (DBTH) demonstrated just how powerful this approach can be. In 2018, by simply introducing a structured wound cleansing protocol, their infection rate plummeted by an impressive 48%. The following year, they added mechanical debridement to the protocol, and infections dropped to just 1.3%—an incredible 82% total reduction. You can read the full details of this successful project on wounds-uk.com.
The takeaway is clear: A systematic, evidence-based approach to bioburden management produces dramatically better outcomes. It’s about using the right agent at the right time—reserving potent systemic antibiotics for spreading or deep tissue infections where they are truly needed.
Selecting Dressings Based on Function
One of the most significant and important shifts in modern wound care is moving from a product-first to a function-first mindset when choosing dressings. Don’t start by asking, “What product should I use?” Instead, ask the more critical question, “What does this wound need right now to move to the next stage of healing?”
The answer comes directly from your comprehensive TIME assessment.
- Is the wound bed dry and desiccated? It needs moisture. A hydrogel is designed to donate moisture and rehydrate the tissue, promoting autolytic debridement.
- Is it draining heavily with high levels of exudate? It needs absorption. An absorptive foam, alginate, or superabsorbent polymer dressing will manage the exudate, lock it away, and protect the surrounding skin from maceration.
- Are you trying to support autolytic debridement on a wound with minimal drainage? It needs a moist, occlusive environment. A hydrocolloid or transparent film is built for that specific job.
This function-first thinking prevents the common and costly mistake of applying the wrong type of dressing—an error that can easily set healing back by weeks. If you want to go deeper, you can explore these 10 evidence-based wound dressing selection strategies.
Validated Adjunctive Therapies
Sometimes, standard debridement and dressings aren’t enough to get a stalled wound moving. Many adjunctive therapies have strong evidence backing them for specific wound types, working alongside primary care to address the underlying physiological issues that are preventing healing.
For instance, compression therapy is the undisputed cornerstone of care for venous leg ulcers. Decades of robust research have proven that applying sustained, graduated compression reduces edema and improves venous return, directly attacking the root cause of the ulcer. Without effective compression, even the world’s most advanced dressing is likely to fail.
Similarly, offloading is non-negotiable for the successful treatment of diabetic foot ulcers. The evidence is overwhelming: reducing pressure on the ulcerated area is the single most critical factor for healing. Whether it’s a total contact cast, a removable cast walker, or another device, the primary goal remains the same—get the pressure off the wound. These therapies aren’t optional add-ons; they are essential, evidence-based components of any comprehensive care plan.
Implementing Clinical Pathways In Your Practice
Knowing the evidence is one thing. Actually putting it into practice consistently, at every bedside with every patient, is where the real magic happens. This requires a strategic shift away from individualized, one-off clinical decisions and moving toward standardized, team-wide processes. That’s the entire purpose of clinical pathways—they are structured, evidence-based frameworks that guide how you care for specific conditions, ensuring every patient receives the same high standard of treatment.
Think of it as your clinic’s official playbook. Instead of every clinician running a different play based on personal preference, the entire team follows a coordinated, evidence-backed plan that has already been proven to work. This is how you transform evidence-based wound care from a theoretical concept into a practical, everyday reality and build a predictable system for achieving better outcomes.
Building Your Evidence-Based Playbook
Putting a clinical pathway in place isn’t about creating more burdensome paperwork. It’s about simplifying and standardizing care so that doing the right thing becomes the easiest and most logical thing to do. It all starts with a few foundational steps that create a structure for sustained success.
First, create a wound care formulary. This is a curated list of approved dressings and products that have been chosen based on solid evidence of their function and cost-effectiveness, not just brand loyalty or historical preference. When you streamline the number of products you use, you reduce clinician confusion, save money through bulk purchasing, and ensure your team becomes experts in using dressings that genuinely work.
Next, you’ll want to design standardized documentation templates. These are more than just records; they are active clinical tools. A well-designed template guides clinicians to capture the most critical data at every visit—such as wound measurements, tissue type percentages, and exudate levels—which in turn drives treatment decisions that align with established frameworks like TIME.
Finally, regular team training and education is absolutely non-negotiable. This critical step gets everyone, from your most experienced nurses to your medical assistants, on the same page about why these new pathways are important. When your whole team speaks the same clinical language and follows the same evidence-based protocols, patient care becomes consistent, safe, and seamless.
Overcoming Barriers to Change
Let’s be realistic—implementing any new system is bound to have its challenges. The biggest hurdle is almost always resistance to change, fueled by the classic “but we’ve always done it this way” mentality. The most effective way to overcome this is to demonstrate the value of the new approach with clear, undeniable data.
Share the outcomes. Show how the new pathways are boosting healing rates, shortening treatment times, or cutting supply costs. Use a compelling case study to illustrate how a standardized approach prevented a serious complication. When your staff sees the tangible positive impact on their patients and their own workflow, getting buy-in becomes exponentially easier.
A successful clinical pathway doesn’t just list steps to follow; it empowers clinicians by giving them a clear, logical, and evidence-backed roadmap. It cuts through the noise of product marketing, supports sound clinical judgment, and builds confidence and consistency across the entire team.
The need for this kind of structured approach is glaring. An international consensus project in 2020/21, validated by 62 specialists, painted a stark picture of the status quo: clinicians reported that only 52% of their chronic wound patients were actually healing, and another 26% had wounds that were not healing at all. But here’s the crucial finding: the same project found that 84% of specialists agreed that implementing evidence-based pathways leads to shorter healing times, less clinical variation, lower costs, and less burden on healthcare professionals. You can read the full consensus findings on woundsinternational.com.
Key Components of an Effective Pathway
To build a pathway that actually gets used and delivers results, make sure it includes a few core elements that guide care from the first visit to the last. A solid pathway is a living document that can be updated as new evidence emerges.
Your clinical pathway should include:
- Clear Assessment Criteria: Spell out exactly what information needs to be collected during initial and follow-up assessments, which should align perfectly with your standardized documentation templates.
- Decision Trees for Interventions: Create simple, easy-to-follow “if-then” logic. For example, “If the wound bed has >50% slough and the patient has adequate blood flow, then initiate enzymatic or sharp debridement.”
- Product Selection Guide (Formulary): Link your wound care formulary directly to the pathway. For instance, “If the wound has moderate to heavy exudate, then select a dressing from the ‘High Absorbency’ category in the formulary.”
- Defined Follow-Up Schedule: Standardize how often patients need to be seen based on their wound type, severity, and the interventions being used. This ensures no one falls through the cracks.
When you develop these practical, clinician-friendly tools, implementing evidence-based care stops being a daunting, abstract idea and becomes a manageable, achievable project. And the returns—in better patient outcomes, smoother workflows, and more engaged staff—are more than worth the initial effort.
How Technology Upholds Evidence-Based Practices

Clinical guidelines and pathways are invaluable in theory, but their real magic happens when they are actually used—consistently, with every patient, every single day. This is where modern technology makes all the difference. It takes those well-intentioned protocols off the shelf or out of a binder and turns them into living, breathing tools that actively guide care at the bedside.
Think about it. Traditional paper charting is a recipe for inconsistency and incomplete data. A missed measurement here, a vague tissue description there, and suddenly a critical care plan is being built on shaky, unreliable ground. Digital platforms are designed to prevent exactly this by weaving evidence-based wound care practices right into the daily clinical workflow.
Instead of depending on human memory or flimsy paper checklists, clinicians are guided by a smart system that knows what to ask and when. It prompts for the critical data points and makes following the right steps the easiest and most efficient path. In this way, technology becomes the guardian of best practices, ensuring every action aligns with what the evidence tells us works best.
Automating Objectivity and Precision
Let’s be honest: one of the biggest and most persistent hurdles in wound care has always been subjectivity. Two different clinicians can look at the same wound and describe it in two different ways, using different terms, making it nearly impossible to track progress accurately over time. Technology brings a level of objectivity and precision to the table we simply couldn’t achieve before.
For instance, modern platforms use AI-powered wound measurement to take the guesswork completely out of sizing. A clinician can simply snap a photo with a tablet, and the system instantly and accurately calculates the length, width, surface area, and even depth. This provides a clean, repeatable data point that tracks healing far more reliably than any paper ruler ever could.
This same AI-driven approach can analyze tissue composition within the wound bed, quantifying the exact percentage of healthy granulation tissue versus slough or eschar. Over time, this objective data creates a crystal-clear, graphical picture of whether a wound is healing, stalled, or getting worse, empowering clinicians to adjust the care plan with confidence backed by hard data.
Capturing Richer Data at the Bedside
Documentation often feels like an administrative chore that pulls clinicians away from their real job: caring for patients. Technology is starting to flip that script, making the process faster, simpler, and surprisingly more detailed and clinically relevant.
A dedicated wound care platform doesn’t just digitize old paper forms; it reimagines the entire documentation process from the ground up. It integrates smart tools that support, rather than interrupt, the natural flow of a patient encounter.
Features like voice-to-text documentation are a prime example. Clinicians can capture detailed, narrative observations in real time just by speaking into their device. This “ambient listening” approach means all those subtle but important clinical insights from the bedside get recorded accurately without anyone having to stop and type. The system can then parse and organize these notes automatically, ensuring all the necessary structured data fields are populated correctly.
From Documentation to Reimbursement
The significant payoff from better technology doesn’t stop at the bedside; it extends directly to the financial health of the practice. We all know that spotty, inconsistent, or incomplete documentation is a primary reason for claim denials and payment delays, which can create a huge operational headache and impact revenue.
Modern wound care systems tackle this problem head-on with automated coding and billing support. By analyzing the structured data captured during the visit, the platform can:
- Suggest the correct CPT and ICD-10 codes based on the documented procedures, wound characteristics, and diagnoses.
- Flag missing information that could cause a claim to be rejected—before it’s even submitted.
- Package a clean, compliant claim that’s ready for submission, drastically cutting down on manual work, human error, and the need for rework.
This powerful integration ensures that the high-quality, evidence-based care you’re providing gets reimbursed accurately and on time. It creates a seamless connection between clinical excellence and operational strength. To see how this works in practice, you can learn more about how AI workflows drive clinical excellence in our detailed article.
By embedding clinical pathways, standardizing data capture, and smoothing out the revenue cycle, technology makes evidence-based practice the default standard of care, not just an aspirational goal.
Measuring Success And Driving Continuous Improvement
Putting evidence-based wound care into practice isn’t a one-and-done project. It’s a living, breathing process of continuous refinement and improvement. Simply rolling out new protocols isn’t the end game. To truly see transformative results, you must measure the impact of those changes and use that data to keep getting better, thereby building a culture where quality is always the north star.
This is about moving past gut feelings and anecdotal wins to focus on hard, objective data. When you consistently track the right key performance indicators (KPIs), you can definitively prove the value of your program, pinpoint areas where you’re falling short, and make smarter, data-driven adjustments. It’s the critical difference between hoping your program is improving and knowing exactly how and by how much.
Key Metrics for Wound Care Programs
To get a truly comprehensive story of your program’s performance, you need to look at a balanced mix of clinical, operational, and patient-centered metrics. Each piece of data tells a different part of the story, and together they provide a complete, 360-degree view of your program’s health and impact.
Clinical Outcomes:
- Healing Rates: This is the ultimate benchmark. You need to be tracking the percentage of wounds that heal completely within a defined timeframe, stratified by wound type.
- Time to Heal: What’s the average number of days it takes for different types of wounds to close? A downward trend in this metric is a clear sign of more effective care.
- Infection Rates: Keep a close eye on the incidence of new wound infections within your patient population. A drop in this number is a powerful indicator that your protocols are hitting the mark.
- Recurrence Rates: For chronic conditions like venous leg ulcers or diabetic foot ulcers, you must track how many wounds reopen after initial healing. A low recurrence rate proves your care plans are effective for the long haul.
Operational Efficiency:
- Documentation Time: Measure how long your clinicians are spending on charting per patient encounter. Reducing this number means more time for direct, hands-on patient care.
- Claim Denial Rates: What percentage of your wound care claims are being kicked back by payers? A lower rate is a direct reflection of better documentation quality and accurate coding.
- Product Utilization and Cost: Dig into your spending on wound care supplies per episode of care. This helps you ensure your formulary is both clinically sound and cost-effective.
Creating a Culture of Quality
Data is useless if it just sits in a dashboard. The real work begins when you establish a regular rhythm for reviewing these KPIs and turning the insights you learn into concrete action. This creates a powerful feedback loop that fuels constant improvement and innovation.
A great place to start is with regular, systematic chart audits. They’re a quick and effective way to see if your new pathways are being followed consistently or if there are documentation gaps. The goal here isn’t to play “gotcha” with your staff, but rather to identify opportunities for additional training and support where it’s needed most.
Success in evidence-based wound care isn’t defined by acing a single metric. It’s about the whole picture: faster healing, smoother operations, lower costs, and, most importantly, a better experience and quality of life for the patient. This data-driven mindset is what keeps your program at the forefront of quality care.
And don’t forget the immense power of patient-reported outcomes (PROs). Metrics like pain levels, functional ability, quality of life, and overall satisfaction provide a crucial perspective that purely clinical data alone cannot capture. When you tie solid data analytics directly to your clinical practice, your team can clearly demonstrate its value and ensure your services evolve right alongside the very latest evidence.
Frequently Asked Questions
Making the significant shift to evidence-based wound care is a major step, and it naturally brings up important questions for everyone involved—from the clinicians at the bedside to the administrators managing the bottom line. Let’s tackle some of the most common ones we hear.
What Is the First Step to Adopting These Practices?
The best and most impactful place to start is right at the beginning: with your assessment process. You can’t effectively treat what you don’t accurately and consistently measure.
Adopting a structured assessment framework like TIME (Tissue, Infection/Inflammation, Moisture, Edge) is the single most powerful first step. It forces a consistent, comprehensive evaluation from every clinician, every single time a wound is seen. This creates a reliable, standardized foundation that makes all the downstream decisions—from debridement techniques to dressing selection—so much clearer, more logical, and defensible.
How Can We Reduce Resistance from Staff?
Change is inherently difficult. The key to getting your team on board isn’t top-down mandates; it’s proving that the new way is demonstrably better for both patients and providers.
Start small with a pilot project. Pick one common wound type you see frequently, such as venous leg ulcers, and meticulously track your outcomes using the new evidence-based protocols. When your team sees healing rates improve, documentation becomes easier, and patient satisfaction climbs, the resistance will naturally melt away. People will always gravitate toward what works and makes their challenging jobs easier.
The goal isn’t just to enforce new rules. It’s to show your team a better way to get the results everyone wants: healthier patients and less chaotic, more predictable workdays. You have to make the right thing the easy thing to do.
What Is the Biggest Mistake to Avoid?
This is an easy one. The most common and costly pitfall we see is getting distracted by shiny new objects—usually the latest and greatest high-tech dressing—while completely ignoring the underlying root cause of the wound.
Think about it: putting an expensive, antimicrobial, silver-impregnated dressing on a diabetic foot ulcer without addressing the constant pressure through proper offloading is a recipe for failure. You’ll go through a lot of costly supplies with absolutely nothing to show for it but a stalled wound. Evidence-based care is holistic. It’s about treating the whole patient and the underlying etiology, not just plugging a hole in the skin.
Ready to tie your clinical and operational workflows together on a single, intelligent platform? Ekagra Health AI helps you embed these evidence-based practices directly into your daily routine, streamlining everything from documentation and coding to billing. See how our end-to-end solution can elevate your practice.
