
An electronic medical record (EMR) system is the digital counterpart to a patient's old paper chart. Think of it less as a simple file and more as the central nervous system of a medical practice, containing the complete medical and treatment history generated within that specific clinic. It replaces the endless rows of filing cabinets with a single, authoritative source of truth, creating a digital hub for all patient care activities within an organization. This foundational technology is not just about storing data; it's about making that data actionable, accessible, and secure for clinicians at the point of care.
From Paper Charts to Digital Powerhouses

The move to an electronic medical record system wasn't just about swapping paper for pixels; it fundamentally rewired how healthcare teams capture, manage, and act on patient information inside their own walls. This transformation marked a pivotal shift from cumbersome, error-prone manual processes to streamlined, data-driven clinical operations.
Not long ago, a patient's story was scattered across dozens of pages in a manila folder. This created huge logistical hurdles. Finding a single lab result or tracking a patient's condition over time meant manually digging through stacks of paper—a slow, frustrating, and error-prone process that consumed valuable clinical time and introduced risks to patient safety. Every handwritten note was a potential point of misinterpretation, and the physical nature of the chart meant it could only be in one place at one time, creating bottlenecks in busy clinical environments.
To see just how much has changed, let's compare the old way with the new.
Paper Charts vs. Digital EMR Systems at a Glance
| Feature | Paper Charts | EMR System |
|---|---|---|
| Accessibility | Single physical copy, locked in a filing cabinet | Accessible instantly by multiple authorized users from various locations |
| Data Retrieval | Manual, slow search through physical pages | Automated, keyword-searchable, instant results for labs, notes, and more |
| Legibility | Dependent on handwriting, often poor and prone to misinterpretation | Standardized, typed text is always clear and unambiguous |
| Data Analysis | Nearly impossible; requires manual abstraction and compilation | Can generate reports, track trends, and flag issues automatically |
| Storage | Requires massive physical space and is costly to maintain | Stored digitally on servers or in the cloud, saving physical space |
| Backup & Security | Vulnerable to fire, flood, theft, and loss | Secured with encryption, access controls, and redundant backups |
This table shows a clear evolution, moving from a fragile, one-dimensional record to a dynamic, multi-user system built for modern care delivery. The transition represents a fundamental enhancement in how patient information is managed, secured, and leveraged to improve care.
The Evolution From Concept to Clinic
The idea of digital records has been around since the 1960s. For decades, however, the technology was so costly and complex that only large government agencies and major hospitals could afford it, and even then, it was mostly used for basic scheduling and billing rather than comprehensive clinical documentation. The vision was there, but the infrastructure was not.
The real shift began when personal computers became common in the 1980s, followed by the internet's explosion in the 1990s. As the hardware became more affordable and powerful, smaller private practices finally had a path to digitize their charts. This grassroots adoption was slow but steady, driven by forward-thinking clinicians who saw the potential for greater efficiency and improved patient care.
What really lit the fire, though, was government action. A major catalyst was the Health Information Technology for Economic and Clinical Health (HITECH) Act of 2009, which offered significant financial incentives for providers to adopt and demonstrate "meaningful use" of certified EMR systems. This single piece of legislation dramatically reshaped the industry in just a few years, turning EMR adoption from a competitive advantage into a near-universal standard of practice.
The core purpose of an EMR is to build a complete, continuous story of a patient's care journey within one practice. It’s the official log of every diagnosis, treatment, and outcome documented by that specific team.
This internal focus is the key difference between an EMR and an Electronic Health Record (EHR). While an EMR is for use within an organization, an EHR is designed to share information between different healthcare providers, creating a longitudinal record of a patient's health across their entire care continuum.
The Impact of Widespread Adoption
The push to go digital has had a massive effect. By 2021, an impressive 88.2% of office-based physicians in the U.S. were using an EMR or EHR system, with 77.8% using a certified platform. This near-total adoption shows that the EMR is no longer a novelty but a standard tool of the trade, especially in outpatient clinics where efficiency and accuracy are paramount.
For a specialty like wound care, this digital backbone is a game-changer. Practitioners can now:
- Instantly pull up a patient's entire wound history, including photos, measurements, and previous treatments.
- Visually track healing progress with hard data over weeks or even months, enabling more objective assessments.
- Make smarter treatment decisions with a complete, organized record at their fingertips, leading to better patient outcomes.
This transition from paper to digital has laid the foundation for a more connected and data-driven future in healthcare. By getting their own house in order with a robust EMR system, practices are better positioned to improve everything from daily operations and financial performance to the quality and safety of patient care. You might be interested in our guide on how EMR systems work in hospitals to learn more.
Getting Work Done: A Look at Core EMR Features
An EMR does so much more than just get rid of your paper charts. It acts as the central nervous system for your entire practice, turning what can often feel like clinical chaos into a smooth, organized flow. To really get a feel for its impact, you have to look past the idea of just "digital records" and see how specific features make each day more efficient, safer, and more collaborative.
Think of an EMR as the engine of a modern clinic. It isn't just a single part but a collection of interconnected tools all working together. Each one is designed to solve a specific administrative or clinical headache, automating the tedious tasks that used to eat up hours. This fundamental shift frees up your team to spend less time shuffling papers and more time focusing on what really matters: your patients. The value of an EMR lies not just in its ability to store information, but in its capacity to streamline workflows and support clinical decision-making in real time.
Let's dive into the core features that make up the backbone of almost every EMR system and see how they play out in a real clinic.
From Check-In to Billing: A Typical EMR Workflow
Imagine a patient arriving at your podiatry clinic for a chronic wound check-up. The second they step through the door, the EMR kicks in, weaving every part of their visit into one seamless digital story. This connected process is what makes an electronic medical record (EMR) system so effective at improving both efficiency and care quality.
Here’s a play-by-play of how these core features work together:
Patient Scheduling: The front desk staff uses the EMR’s built-in calendar to check the patient in. Right away, the system updates the patient’s status from "scheduled" to "arrived," which sends an automatic notification to the clinical team that their next appointment is ready. This simple action eliminates verbal handoffs and keeps the entire clinic aware of patient flow.
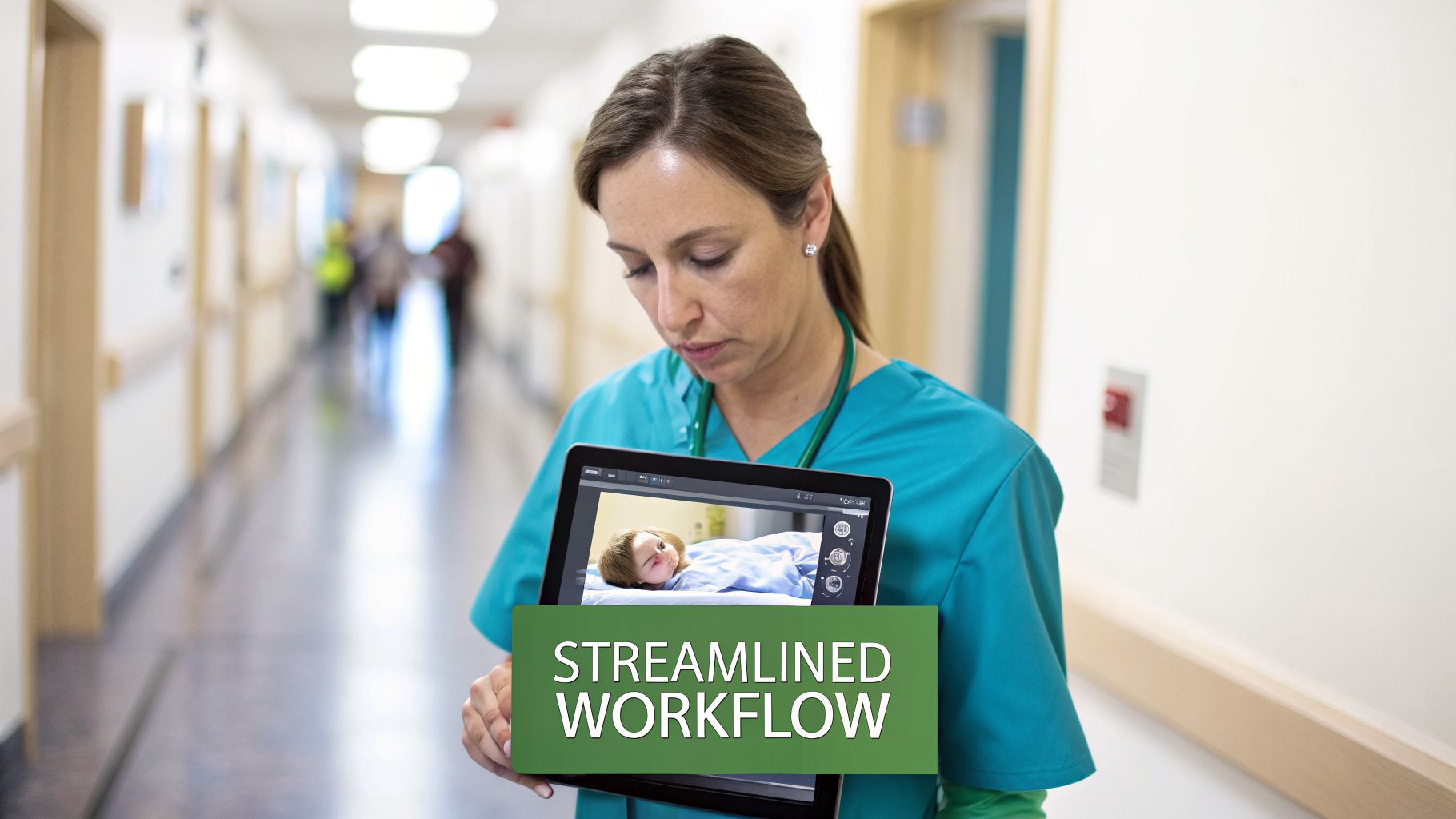
Digital Charting: A nurse guides the patient to an exam room and pulls up their chart on a tablet. Instead of flipping through a thick paper file, she sees a clean, organized dashboard. The patient’s vitals, allergies, medications, and chief complaint are all right there. Every past visit note and wound photo is just a click away, providing immediate context for the current visit.
Order Entry (CPOE): During the exam, the physician decides a new dressing is needed and a lab test should be run. Using the Computerized Provider Order Entry (CPOE) feature, they send these requests digitally—one goes to the supply room, the other to the lab. This gets rid of handwritten orders, cutting down on mistakes from bad handwriting and getting the ball rolling much faster. Orders are legible, standardized, and time-stamped.
E-Prescribing (eRx): The physician also needs to prescribe a new topical antibiotic. With the e-prescribing module, they can securely send the prescription to the patient’s pharmacy of choice in seconds. The system can also flag potential drug interactions or allergies, adding a critical layer of safety. It's faster, more secure, and helps eliminate the medication errors that can happen with handwritten scripts.
This whole sequence shows how an EMR weaves a single, unbroken thread of information. Every action is logged in real-time, building a complete and accurate record of the visit from start to finish. This digital trail not only improves patient care but also provides a robust record for billing and compliance purposes.
Core Features That Power Modern Clinics
While the user interface might look different from one system to another, most EMRs are built around the same set of essential tools. These features are there to handle the most common jobs in any healthcare setting, from back-office admin to hands-on clinical care. Understanding these components is key to evaluating different systems.
A modern EMR doesn't just store information; it actively helps you manage it. By integrating tasks like scheduling, charting, and ordering, the system reduces administrative friction and allows clinicians to work more efficiently.
Here are some of the key features you'll find:
- Patient Demographics and Insurance: This is your central hub for all non-clinical patient data. It holds everything from contact info and insurance details to emergency contacts, making sure your billing information is always accurate and easy to find. This integration ensures that administrative and clinical data are seamlessly linked.
- Clinical Notes and Documentation: This is the heart of the EMR. It offers structured templates for different kinds of appointments (like an initial consult, a follow-up, or a procedure), which keeps your documentation consistent and thorough. Many systems even have templates designed for specialties like wound care or dermatology, which can drastically improve charting efficiency and quality.
- Reporting and Analytics: A good EMR can transform thousands of individual data points into powerful insights. A clinic manager can run reports to track patient outcomes, see how productive providers are, or spot trends in diagnoses. This data helps shape both business and clinical strategies, enabling practices to operate more like data-informed organizations. To see more on how data can guide clinical work, check out the benefits of clinical decision support systems.
These core functionalities work in concert to create an environment where information flows freely and logically, supporting clinicians and administrators in their daily tasks and long-term goals.
Weighing the Benefits and Challenges of EMR Adoption
Making the switch to an electronic medical record (EMR) system is a massive decision for any practice. It's not just a tech upgrade; it's a fundamental change in how your team documents, communicates, and ultimately delivers patient care. To navigate this transition well, you need a clear-eyed view of both the incredible advantages and the very real hurdles you'll face. The journey requires strategic planning, team buy-in, and a realistic understanding of the road ahead.
The upsides are powerful. Anyone who's spent years working with paper charts knows the struggle—illegible handwriting, misplaced files, and the time wasted just tracking down a patient's history. EMRs bring a level of clarity and efficiency that paper could never offer, making documentation consistent, legible, and instantly available to all authorized users.
This creates a ripple effect across the entire care team. When everyone from the front desk to the clinicians is looking at the same up-to-the-minute information, you eliminate guesswork and reduce communication errors. That shared, centralized record is absolutely essential for keeping everyone on the same page and delivering safe, effective care, especially for patients with complex conditions who see multiple providers.
The Major Wins of Going Digital
The benefits go far beyond just having neater notes. A good EMR system actively helps improve both your clinical quality and your operational workflow. One of the biggest wins is simplified compliance. Modern EMRs are built from the ground up with regulations like HIPAA in mind, embedding features that guide your practice toward meeting those standards through audit trails, access controls, and secure data handling.
Another huge advantage is enhanced data analysis. EMRs turn static patient charts into a dynamic source of insight. You can finally start tracking patient outcomes over time, spotting trends across your patient population (like an increase in a specific type of infection), and measuring your clinic's performance against important quality benchmarks. This data-driven approach is key to participating in value-based care models.
Here’s a quick rundown of the primary benefits:
- Improved Documentation Accuracy: Standardized templates and fields prompt staff to capture all necessary information, which cuts down on ambiguity and the potential for clinical errors. This structured data entry ensures completeness and consistency.
- Faster Access to Patient Information: Clinicians can pull up a complete patient history in seconds, whether they're in the exam room with the patient or on call after hours. This immediate access is critical for making timely and informed decisions.
- Better Care Coordination: Multiple providers within the same practice, even across different specialties, can access and add to the same patient record. This creates a single, unified story of the patient's care, which is critical for anyone with complex health needs.
When you add it all up, these improvements help clinicians make better, more informed decisions and can lead directly to better patient outcomes and increased patient safety.
Navigating the Hurdles of Implementation
Of course, the road to adopting an EMR isn't always smooth. The implementation itself can be a major project, requiring a significant financial investment, careful planning, and a ton of commitment from your team. A common complaint we hear is alert fatigue—clinicians get so many automated notifications and pop-up warnings that they start tuning them out, which carries the risk of them missing a truly critical warning. Additionally, the initial learning curve can temporarily slow down productivity as staff adapt to new workflows.
The most persistent challenge with many EMR systems is the creation of 'data silos.' When a standalone EMR can't communicate with other systems, it locks valuable patient information away, defeating the goal of coordinated care.
Think about a common wound care scenario: a patient is treated at an outpatient clinic for a chronic wound and is later admitted to the hospital for an infection. If the hospital's EMR can't talk to the clinic's EMR, the hospital team is flying blind. They have no idea about the wound's history, what treatments have already been tried, or if it was healing or getting worse. This forces them to start from scratch, leading to redundant tests, delays in care, and real risk for the patient.
This is exactly why interoperability—the ability of different systems to talk to each other—has become the cornerstone of a modern electronic medical record EMR system. The industry is finally moving away from closed, isolated platforms and toward connected solutions that can share data securely. In fact, future trends show that 84% of healthcare organizations will view interoperability as essential for superior patient care by 2026. This push is already yielding results in the U.S., where 81% of hospitals now give patients app-based access to their health information, a direct result of improved data-sharing capabilities. You can read more about these key healthcare trends on riomed.com.
How to Choose the Right EMR for Your Practice
Picking an electronic medical record (EMR) system is easily one of the biggest technology decisions your practice will ever face. This isn't just about buying software; it's a long-term investment that will fundamentally shape your clinical workflows, administrative load, and even your team's day-to-day happiness for years. With so many vendors out there, each promising to revolutionize your practice, it’s easy to feel overwhelmed. However, you can make the process manageable by breaking it down into a structured, methodical evaluation.
The real key is to look past the flashy sales pitches and get down to what your practice actually needs to function well. A system that’s perfect for a massive hospital could be a clunky, overpriced headache for a small wound care clinic. The right EMR should feel like a natural extension of your team, seamlessly integrating into your daily routines, not another obstacle in the way of great patient care.
Define Your Practice Needs and Goals
Before you even think about looking at a single vendor's website, you need to look inward. The first and most critical step is to map out your practice's specific needs. Where are the biggest bottlenecks in your workflow right now? What administrative tasks are eating up your team's valuable time? What are your long-term clinical and business goals?
Getting everyone involved in this conversation is crucial—from your physicians and nurses to the front desk staff and billers. This teamwork helps build a clear checklist of "must-haves" versus "nice-to-haves" and ensures the chosen system will meet the needs of all users, not just one group.
- Specialty-Specific Templates: Does the EMR offer documentation tools built for your specialty? A podiatry or wound care clinic has very different charting needs—like specific fields for measurements, tissue types, and treatment plans—that a generic EMR simply won’t accommodate effectively. Ask for demos of these specific features.
- Scalability for Growth: Think about where your practice might be in five or ten years. The electronic medical record EMR system you choose should be able to grow with you, whether you’re adding providers, opening new locations, or offering more services. A scalable system prevents you from having to go through this entire process again in a few years.
- Workflow Integration: Carefully map out your current patient journey, from check-in to billing. How well would a new EMR fit into this flow, and where could it improve things? The goal is to make the technology work for you, not force your practice to conform to the software's rigid structure. A great EMR should adapt to your best practices.
Assess the Total Cost of Ownership
The initial price tag on an EMR is just the tip of the iceberg. To avoid getting hit with unexpected bills later, you need to calculate the Total Cost of Ownership (TCO). This gives you a much more realistic picture of what you'll actually be spending over the long haul and is essential for accurate budgeting.
Don't be swayed by a low initial price. A "cheaper" system with high recurring fees for support, training, or essential modules can quickly become the more expensive option over its lifespan.
To get a true sense of the TCO, look beyond the subscription fee and factor in these potential costs:
- Implementation and Data Migration Fees: The cost to get the system set up and move over all your existing patient data from paper or a previous system. This can be a significant one-time expense.
- Hardware Requirements: Will you need to buy new servers, computers, or tablets to run the software effectively? Ensure your current hardware meets the vendor's specifications.
- Training Costs: Budget for both the initial training for your current team and ongoing training for new hires. Inadequate training is a leading cause of poor EMR adoption.
- Ongoing Support and Maintenance Fees: These are typically monthly or annual contracts for technical support and essential software updates. Understand what level of support is included.
- Customization and Integration Costs: The price for connecting the EMR to other critical systems, like labs, imaging centers, or your billing software.
Deciding between hosting the EMR on your own servers versus using a cloud-based solution is a major part of the cost and maintenance equation. Each model has its own set of pros and cons that can significantly impact your TCO and day-to-day operations.
Here's a breakdown to help you compare the two primary deployment models:
On-Premise vs Cloud-Based EMR Deployment Models
| Factor | On-Premise EMR | Cloud-Based EMR |
|---|---|---|
| Initial Cost | High upfront investment for servers, hardware, and software licenses. | Lower initial cost with a monthly or annual subscription fee. |
| Maintenance | Your internal IT team is responsible for all maintenance, security, and updates. | The vendor manages all updates, backups, and server maintenance. |
| Accessibility | Access is typically restricted to the local network within the practice. | Accessible from any device with an internet connection, anywhere. |
| Security | You are fully responsible for data security, backups, and HIPAA compliance. | Vendor manages security infrastructure, often with dedicated experts. |
| Scalability | Scaling up requires purchasing new hardware and can be costly and slow. | Easy to scale by adjusting your subscription plan as you grow. |
Ultimately, cloud-based EMRs have become the standard for most modern practices due to their lower upfront costs, easier maintenance, and greater flexibility. However, larger organizations with robust IT departments may still prefer the control offered by an on-premise solution.
Verify Certification and Security
This part is absolutely non-negotiable. Any EMR system you seriously consider must be ONC-Health IT Certified. This certification is your assurance that the system meets strict federal standards for functionality, security, and the ability to share data with other systems (interoperability). It's also a prerequisite for participating in many federal incentive programs and value-based care initiatives.
Security and certification go hand in hand. Protecting patient data is paramount, so your vendor must demonstrate rock-solid security protocols. This includes data encryption both in transit and at rest, regular backups, disaster recovery plans, and role-based access controls to ensure sensitive information is protected. It also means using tools like HIPAA-compliant online forms for patient intake to maintain security at every touchpoint.
On that note, streamlining your financial processes is just as important. You might find our guide on medical coding automation tools helpful for boosting your practice’s revenue cycle efficiency.
Run Effective Demos and Check References
Once you have a short list of potential vendors, it's time to schedule demos. Don't think of these as sales pitches; treat them like a test drive. Come prepared with a list of real-world scenarios that happen in your practice every day. Give the salesperson your most common and most complicated workflows.
Ask the vendor to walk you through a typical patient encounter for your specific field. For instance, have them show you how a home health nurse would document a wound assessment—including uploading a photo and ordering supplies—all from a tablet in the patient's home. See how many clicks it takes. Is the interface intuitive or confusing?
Finally, always ask for references from practices that are similar to yours in size and specialty. And when you call them, be direct. Ask them about their real experience with implementation, how responsive the support team is, and what impact the EMR has truly had on their daily work. Ask them what they wish they knew before they signed the contract. This unfiltered feedback is often the most valuable information you can get.
The Next Frontier: AI Platforms Beyond the EMR

The electronic medical record emr system was a huge leap forward, getting practices off paper and into the digital age. But at its core, an EMR is still just a sophisticated database—a place to store information. It excels at capturing data but often falls short in helping clinicians interpret it or reduce their administrative burden. What if your EMR could do more than just hold data? What if it could help you make sense of it, lighten your workload, and get you paid faster?
This is exactly where the next wave of health technology is heading. New AI-powered platforms aren't trying to replace your EMR. Instead, they work right alongside it, acting as an intelligent layer that transforms that passive digital filing cabinet into an active, intelligent partner in care.
Think of it this way: Your EMR is a perfectly organized library. It has every patient chart filed correctly, but you still have to go in, pull each book, and read through it to find what you need. An AI platform is like having a brilliant research assistant who reads the charts for you, highlights the critical information, drafts a summary before you even sit down, and points out connections you might have missed.
Making Your EMR Work Smarter, Not Harder
AI platforms like Ekagra Health AI are built to tackle the biggest headaches that come with EMRs—namely, the overwhelming documentation burden and the tangled, tedious process of medical coding. They do this by layering smart automation on top of the system you already use, enhancing its capabilities without requiring a complete overhaul of your existing infrastructure.
Instead of wrestling with clunky templates and an endless sea of checkboxes, these platforms offer a much more natural, human-first way to work. This is where ideas that once felt like science fiction—like a conversation automatically turning into a complete clinical note—are quickly becoming a clinical reality.
The goal of AI in healthcare is not to replace the clinician but to remove the administrative barriers that stand between them and their patients. By automating repetitive tasks, AI gives providers back their most valuable resource: time.
This isn't a far-off future; it's happening now. The global hospital electronic health records market is on track to hit $28.94 billion by 2035. This growth is fueling innovations like AI scribes that can listen in and document visits automatically—a major trend expected to take hold by 2026. This aligns perfectly with platforms designed to connect the entire process, from a spoken conversation during a patient encounter to a submitted claim, creating a truly seamless workflow.
Key AI Capabilities Enhancing the EMR
These next-generation platforms aren't just a single feature. They are a suite of connected tools that bring automation and intelligence to every part of the patient encounter. They’re designed to solve practical, real-world problems and deliver a tangible return on investment, especially in documentation-heavy fields like wound care.
Three core capabilities really stand out:
Ambient Clinical Documentation: Imagine having a normal, natural conversation with your patient, without ever needing to turn to a keyboard. Ambient AI technology listens quietly in the background, capturing the dialogue and automatically creating a structured, comprehensive clinical note in real time. The system is smart enough to identify and organize the patient’s history of present illness, exam findings, and your treatment plan, filling out the EMR note so all you have to do is a quick review and edit before signing off.
AI-Powered Image Analysis: In wound care, accurate measurements are everything, but they can be subjective and time-consuming. AI changes the game completely. A clinician can just snap a photo of a wound with a phone or tablet, and the AI platform instantly analyzes it. It provides precise, objective measurements of length, width, and surface area, identifies different tissue types (like granulation or slough), and can even track healing progress over time by comparing images. The annotated image is then attached directly to the patient's chart in the EMR, creating a rich visual record.
Automated Medical Coding: Once the note is finalized, the platform's AI engine gets to work again. It reads through the documentation—including the structured text and transcribed conversation—and suggests the right CPT and ICD-10 codes for the visit. This transforms a complex, manual task that often requires a certified coder into a quick, automated step. By ensuring the codes perfectly match the documentation, it slashes coding errors, reduces claim denials, and speeds up the entire revenue cycle.
From Voice to Claim in Minutes
When you put all these pieces together on a single platform, you create a fluid, end-to-end "voice-to-claim" process. The encounter starts with a conversation and ends with a clean, coded claim ready for billing—often in a fraction of the time it used to take. This hyper-efficient workflow eliminates the delays and handoffs that plague traditional processes.
This unified approach is what really separates these platforms from a traditional electronic medical record EMR system. They create a closed loop where clinical documentation directly and automatically fuels the revenue cycle, bridging the gap between providing patient care and getting paid for it. As EMRs continue to evolve, integrating technologies like AI-driven data extraction from documents is becoming essential for making sense of all this information and improving how a practice operates.
For busy wound care teams, this all adds up to less time buried in administrative work and more time focused on what matters: delivering excellent patient care. It’s about finally turning all that data into action, improving both clinical outcomes and the financial health of the practice.
A Few Common Questions About EMR Systems
As you consider bringing an electronic medical record EMR system into your practice, you're bound to have some questions. It’s a big decision with long-term implications for your staff and patients. Let's tackle a few of the most common ones we hear from clinicians and practice managers to help clear things up and provide greater clarity.
What Is the Main Difference Between an EMR and an EHR System?
This one comes up all the time, and it really boils down to how the information is shared and the scope of the patient record.
An Electronic Medical Record (EMR) is the digital version of a patient's chart from a single practice or organization. Think of it as the complete, detailed story of the care a patient gets from you and your team. It's an internal record, optimized for your specific workflows, diagnosis, and treatment within your four walls.
An Electronic Health Record (EHR), on the other hand, is designed to be shared. It includes everything you'd find in an EMR, but it's built with interoperability in mind to connect with other healthcare providers. An EHR creates a comprehensive, long-term picture of a patient's health by pulling together records from their family doctor, specialists, labs, hospitals, and other care settings.
Here's a simple way to think about it: An EMR is a patient's story written by one author (your practice). An EHR is that same story told by a team of authors (all their providers), creating a much richer and more coordinated narrative that follows the patient wherever they go.
While an EMR is fantastic for improving how things run within your four walls, an EHR is what makes true, collaborative care possible across the entire health system. Most modern systems today offer EHR capabilities, even if they are sometimes referred to as EMRs.
How Secure Is Patient Data in an Electronic Medical Record EMR System?
Protecting patient data isn't just a feature; it's the foundation of any legitimate EMR, and it's heavily regulated by the Health Insurance Portability and Accountability Act (HIPAA). Any reputable EMR vendor uses a layered, defense-in-depth approach to keep sensitive information locked down.
You should expect to see security measures like these:
- Data Encryption: This scrambles patient data using complex algorithms, making it completely unreadable to anyone without authorization, both when it's stored on a server ("at rest") and when it's being sent over a network ("in transit").
- Role-Based Access Controls: This is a critical one. It means your staff can only see the patient information they absolutely need to do their jobs. A front-desk scheduler, for instance, shouldn't be able to access a patient's clinical notes or past medical history.
- Comprehensive Audit Trails: Every single click and action inside the EMR is tracked—who viewed a chart, who edited a note, what was changed, and exactly when they did it. This creates a powerful trail of accountability and is essential for security investigations.
If you opt for a cloud-based EMR, the data is typically stored in highly secure, HIPAA-compliant data centers with physical and digital security protocols that go far beyond what an individual practice could ever implement on its own. Choosing an ONC-Certified EMR provides another level of assurance that the system meets strict federal standards for security and privacy.
How Long Does It Typically Take to Implement an EMR System?
There's no single answer here, as the timeline really depends on the size of your practice, the complexity of the system you choose, how much data needs to be migrated, and how ready your team is for the change.
For a small, independent clinic with maybe one to five providers, a straightforward cloud-based EMR can often be up and running in 4 to 8 weeks. This timeline usually assumes minimal customization and a motivated team.
For larger practices, hospital departments, or multi-location groups, the process is more complex and can easily take 3 to 6 months, sometimes longer. This extended timeframe accounts for more detailed workflow analysis, custom template building, integration with other systems (like labs and billing), and phased training schedules.
Implementation is much more than just flipping a switch. It’s a full-blown project that includes configuring the system to your needs, migrating data from old paper or digital records, training your entire staff, and having dedicated support during the "go-live" week. A successful launch hinges on careful planning, strong project management, and getting everyone on board with the new way of working.
Can an EMR System Really Help Improve Our Clinic's Revenue Cycle?
Yes, absolutely. A well-chosen and properly implemented EMR can have a major, positive effect on your clinic's finances by cleaning up several key steps in your revenue cycle.
First, it nails down charge capture. Because documentation and billing are connected within the same system, the EMR helps ensure every single billable service, procedure, and supply is captured right at the point of care. That alone can stop significant revenue from slipping through the cracks.
Second, it dramatically improves coding accuracy. Many EMRs use structured templates and built-in prompts that guide clinicians to include all the specific details needed for proper coding. This cuts down on the back-and-forth with billers and reduces the risk of claim denials due to insufficient documentation.
This is where adding an AI-powered platform to your EMR can be a game-changer. The AI can analyze clinical notes in real time to suggest the correct CPT and ICD-10 codes, spot potential compliance issues before a claim is submitted, and basically fast-track the entire journey from documentation to payment.
By making it easier to submit clean claims electronically the first time, a good EMR shortens your payment cycle, reduces the administrative load on your billing team, and directly strengthens your practice's bottom line. It transforms the revenue cycle from a reactive, manual process into a proactive, data-driven one.
Ready to see how AI can transform your wound care practice, turning documentation burdens into a seamless, voice-to-claim workflow? Ekagra Health AI delivers an end-to-end platform designed by clinicians to reduce documentation time by up to 70% and accelerate your revenue cycle.
