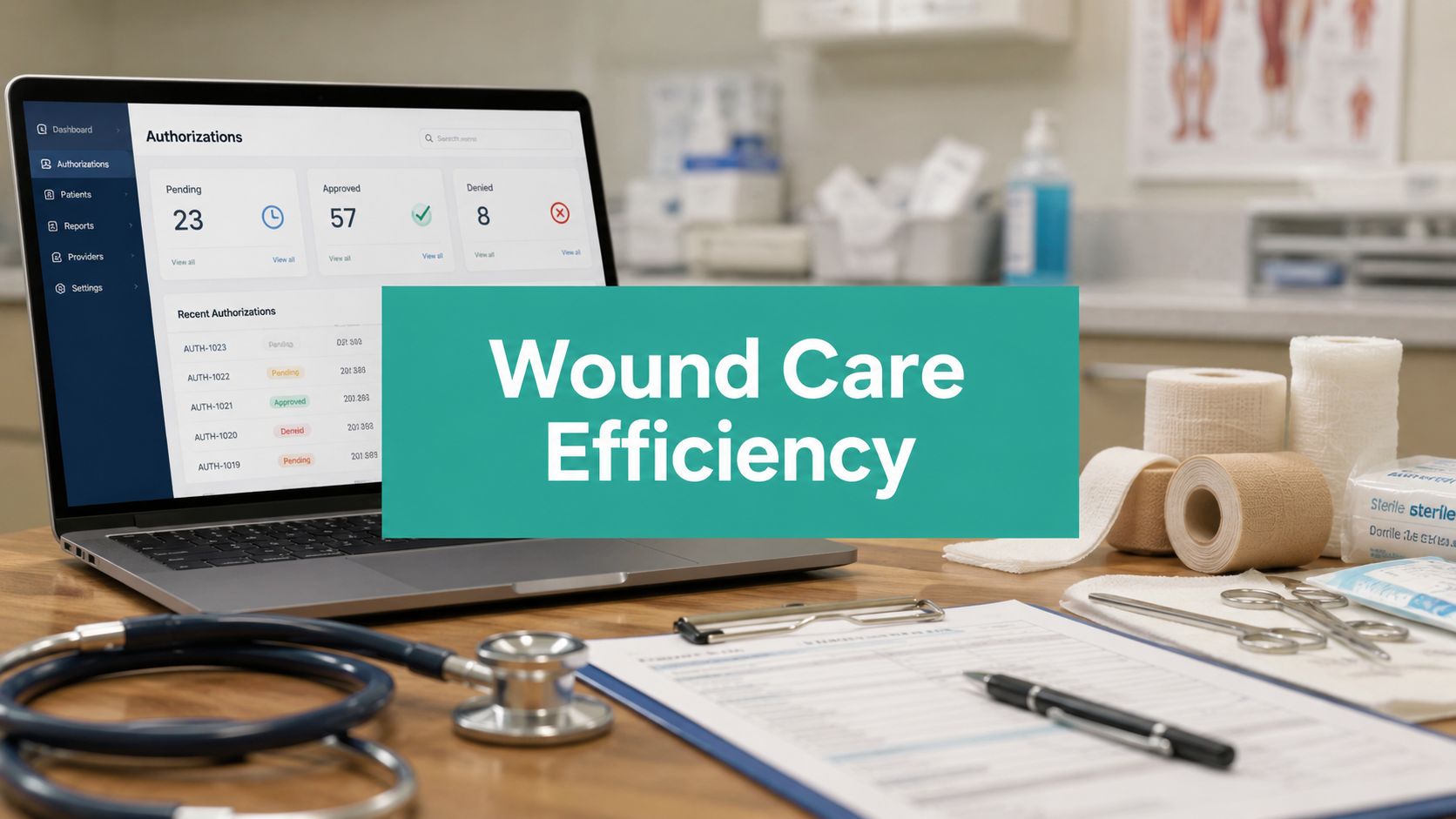
Friday at 4:20 p.m. is when prior authorization failures usually show up in wound care. The chart is done. The wound photos are in. The vascular history is somewhere in the note. The team is trying to get negative pressure wound therapy moving before the weekend, and the payer response comes back with the kind of denial that makes everyone lose time twice: insufficient documentation, medical necessity not established, submit additional records.
That denial usually doesn't mean the treatment was wrong. It means the chart didn't tell the story in the format the payer needed. In wound care, that gap is expensive. Debridement depth, tissue type, exudate character, prior conservative treatment, offloading, vascular status, infection management, serial measurements. Miss one element, and the whole request can stall.
The Friday Afternoon Prior Authorization Problem
A common version of this mess starts with a diabetic foot ulcer. Wagner grade documented vaguely. NPWT requested after debridement. The note says “significant slough” but never states the percentage. Drainage is described as “moderate” but not whether it's serous, serosanguinous, or purulent. The payer wants proof that standard care was tried and failed, plus wound dimensions over time, plus the reason advanced therapy is medically necessary now. The nurse has part of that in the intake. The physician dictated another piece. Billing has to chase the rest.
That's how clinics end up doing prior auth work three times. Once to submit, again to answer a denial, and a third time to appeal something that should've gone through the first pass.
The burden isn't anecdotal. Prior authorization now consumes roughly 13 hours of staff time per week for physicians, with an average of 39 requests submitted weekly. This wastes about $11,000 per clinician annually, and 94% of doctors report that these delays have negatively impacted clinical outcomes, according to the AMA's prior authorization reporting.
What manual wound care workflows get wrong
Manual processes fail in predictable places:
- The chart is clinically accurate but administratively incomplete. A strong wound assessment may still miss the exact payer trigger needed for approval.
- Key details live in different places. Surface area may be in the photo log, debridement detail in the procedure note, and prior failed care in an earlier visit.
- No one catches the omission before submission. The payer catches it later, after treatment is delayed.
Practical rule: If your team is still relying on memory to know which payer wants which wound detail for which service, the process is already too fragile.
That's why I don't see prior authorization software as another admin layer. I see it as a control system. Clinics that are reworking denials every week should spend time studying Ekipa AI's workflow automation insights, not because automation sounds nice, but because wound care margins disappear when staff keep doing avoidable rework.
Why this hits wound care harder
Wound care has unusually dense documentation requirements. A debridement note isn't just a procedure note. It supports coding, medical necessity, product use, and often the next authorization. When that foundation is weak, the clinic doesn't just lose time. The patient may lose treatment momentum over a weekend or longer.
How Prior Authorization Software Actually Works
At 4:30 on a Friday, the nurse has finished the dressing change, the provider has documented the debridement, and the billing lead is trying to send an authorization before the office closes. The note says the wound is improving. The payer wants proof of prior conservative care, current measurements, tissue type, and a clear reason the next service is medically necessary. If those details are scattered across the chart, the request goes out weak or does not go out at all.

Prior authorization software fixes that operational gap by pulling the chart into one review path before staff submit anything. In a wound clinic, that means the system reads structured fields such as diagnosis codes, procedure intent, wound size, laterality, and visit history, then checks the narrative note for the details that often decide whether a request survives payer review. I have seen denials triggered by omissions as small as missing debridement depth, no documentation of failed standard care, or a product request that was never tied to the wound's current condition.
A useful workflow usually has four parts:
Chart intake
The software gathers the clinical and administrative pieces already documented in the record. That can include wound measurements, staging or severity language, prior treatment history, CPT intent, ICD-10-CM diagnosis support, and free-text details from the assessment and procedure note.Payer rule check
The request is matched against payer-specific criteria before submission. For wound care, that often means checking whether the chart supports medical necessity for debridement, negative pressure wound therapy, skin substitute use, or another advanced intervention.Documentation gap alerts
The system flags missing or weak elements while the patient story is still fresh. Common examples include no tissue description, no pre and post procedure measurements, no ulcer duration, no record of conservative care, or a diagnosis that does not support the service requested.Electronic routing and status tracking
Once corrected, the request is submitted electronically and tracked inside the clinic workflow so staff are not hunting through faxes, portals, and voicemail.
The practical value is not automation for its own sake. It is earlier failure. If the request is going to break, it should break in your office while the provider can still add the missing wound bed description or clarify why standard care was not enough.
The better systems also fit into the work queue staff already use. That matters more than feature lists. If nurses have to document in one place, billers in another, and providers in a third portal, adoption falls fast. Clinics should evaluate implementing electronic prior authorization based on whether it cuts rework inside the existing EHR process, not whether the demo looks polished.
I look for software that behaves like a documentation checkpoint tied to clinical logic. A request for advanced wound treatment should prompt the same questions an experienced reviewer would ask. Is the wound size documented? Has the wound stalled? Is there evidence of infection control, offloading, compression, or other standard treatment where appropriate? Tools built with clinical decision support for healthcare workflows in mind tend to handle that review better because they connect the authorization task to the clinical record instead of treating it like a billing afterthought.
What the software cannot do is rescue weak care or override a payer policy exclusion. It can, however, stop avoidable denials caused by vague phrases like "wound improving" when the chart never states the actual trajectory, tissue burden, drainage pattern, periwound condition, or reason an advanced service is being requested now.
Connecting Software to Clinical Triggers and Codes
In wound care, prior authorization software earns its keep when it ties the request to the exact clinical trigger the payer expects. That's where generic automation falls short. Wound services are code-driven, but approval decisions are chart-driven.

Debridement requests
Take CPT 11042 through 11047. The code selection depends on depth and surface area. If the note supports subcutaneous debridement but never clearly states the depth reached, the request is vulnerable. If necrotic tissue is mentioned without describing what was removed, the payer may treat the procedure note as incomplete.
A useful system checks whether the chart connects:
- Procedure depth to the selected debridement code
- Tissue description such as slough, eschar, fibrin, or devitalized tissue
- Measurements before and after debridement
- Relevant diagnosis support such as chronic ulcer coding and wound severity details
One example from practice is a chronic lower extremity ulcer documented with ICD-10-CM L98.499. If the note says only “chronic ulcer with drainage,” that's weak. If it states wound bed percentage, debridement depth, exudate type, odor, and periwound maceration, the request is much harder to challenge.
NPWT requests
Negative pressure wound therapy denials often come from an incomplete bridge between wound severity and treatment progression. The issue usually isn't that NPWT is unreasonable. It's that the record doesn't establish why standard care isn't enough.
Prior authorization software can flag a request when the note is missing the elements that matter most in this setting:
- Prior course of care and whether the wound failed to progress
- Serial measurements showing stagnation or inadequate improvement
- Wound bed and exudate details
- Associated factors such as offloading, edema control, vascular assessment, or infection treatment
In wound programs, those details are often buried in separate visit notes. Good software pulls them together before the request is sent.
Skin substitutes and advanced biologics
Denials become especially costly at this stage. The request usually rises or falls on whether the chart proves the wound is non-healing despite appropriate treatment. Vague descriptors are a major problem. Survey data cited in a wound care WISeR analysis found that 68% of denials stem from vague clinical descriptors, not lack of treatment need, which is why vague language kills advanced wound product requests so often in real clinics. The same discussion also points out how quantifying Wagner grade, debridement details, and exudate type matters for payer review in the current environment, as outlined in this WISeR-focused wound care documentation guide.
If the note says “wound improving slowly,” the payer hears opinion. If the note shows measured change over time, tissue composition, and failed prior care, the payer sees evidence.
Coding support matters here too. A clinic that wants fewer preventable denials should expect prior auth workflows to align with coding logic. That's one reason wound programs increasingly pay attention to medical coding automation tools for specialty care. The codes and the narrative have to agree.
The New Rules from CMS and What They Mean for Your Clinic
A wound clinic can lose an entire Monday before the first patient arrives. Friday's skin substitute request is still pending. The payer wants more detail on prior conservative treatment, drainage, measurements, and debridement history. Staff spend the morning pulling notes from separate visits, and the patient's treatment plan slips again.
That problem is getting harder to carry with manual workflows because CMS is pushing prior authorization toward faster electronic exchange and greater payer transparency. The CMS Interoperability and Prior Authorization Final Rule is scheduled to require affected payers to support FHIR R4-based prior authorization APIs by January 1, 2027, and to report certain prior authorization metrics earlier, as outlined in this CMS prior authorization update for providers. For a wound program, that means the old method of phone calls, fax packets, and staff memory will keep breaking under tighter response expectations.
The operational point is simple. Clinics need documentation and authorization workflows that can move as fast as the treatment plan. That is one reason many organizations pair intake, coding support, and authorization tracking with healthcare claims management software for revenue cycle control, rather than treating prior auth as a disconnected front-end task.
Why wound clinics should pay attention now
Wound care requests often look routine on paper and urgent in practice. A delay on serial debridement, NPWT continuation, or a skin substitute application can throw off scheduling, prolong open wound time, and create a new round of chart updates because the original note no longer matches the planned service date.
CMS pressure matters here because wound clinics are exposed on both the clinical side and the billing side. If the authorization packet misses the wound measurements from the last two visits, fails to show failed conservative care, or lists a procedure code that does not match the narrative, the denial does not stay in the auth queue. It reaches the schedule, the claim, and the patient.
The next change is more specific to wound programs. The WISeR model is planned to begin January 1, 2026, and skin and tissue substitutes for non-healing wounds are included on the prior authorization list in the model materials, according to this legal analysis of the WISeR model. For clinics that rely on advanced wound products, that raises the cost of loose documentation.
The WISeR model changes the documentation standard
WISeR is planned as a six-year model running from January 1, 2026 through December 31, 2031 in selected states. It is designed to use technology-supported review along with clinician oversight for higher-risk Medicare Part B services. In practical terms, wound clinics should expect closer scrutiny of whether the chart shows the clinical trigger for treatment, not just the intention to provide it.
That has real consequences for common wound scenarios. A note that says “ulcer stable” will not carry a skin substitute request very far if the payer is looking for wound duration, prior standard care, measurements over time, tissue quality, offloading or compression history, and signs of stalled healing. The same applies to debridement. If the record lists debridement but does not document tissue type, depth, method, and medical necessity in a way that supports the billed service, the clinic creates avoidable review risk before the claim is even filed.
This is why clinic directors should treat prior authorization software as a documentation control point, not just an admin tool. In wound care, it needs to catch missing evidence before submission, tie the request to the actual service planned, and keep the chart package consistent across nursing notes, physician documentation, and billing data.
For clinic directors managing shared compliance workflows across locations, especially teams that exchange records across borders or outside the EHR, this essential guide for Canadian healthcare is useful as an operational reference on secure file handling. The regulatory details are Canadian-focused, but the discipline around protected clinical documents applies anywhere records move between staff, reviewers, and billing teams.
Measurable Benefits Beyond Less Paperwork
A wound clinic feels prior authorization failure in three places at once. The treatment calendar slips. Staff spend extra time rebuilding chart packets. Payment slows down after the visit because the same documentation weakness that delayed the authorization often weakens the claim.
In practice, the measurable benefit is control. Good software shortens the time between order, review, and treatment. It also cuts the amount of staff rework needed to chase signatures, attach missing notes, resend photos, and answer payer questions that should have been handled before submission. For a clinic treating chronic ulcers, delayed negative pressure therapy, debridement, or skin substitute placement can easily turn one missed documentation element into a week or two of avoidable drift in care.
Operational gains that matter
Clinic directors usually see the first improvement in staff time. Fewer requests sit in email threads or fax queues. Fewer chart packets come back because one progress note used different language than the procedure note. Fewer callbacks land on the nurse who already documented the wound three visits ago.
The second improvement is cycle time. A software workflow that checks for required fields before submission helps the team send a cleaner request the first time. In wound care, that matters because authorizations often depend on serial measurements, prior conservative treatment, vascular status, offloading or compression history, and procedure-specific support in the note. If any one of those pieces is missing, the clinic loses days.
Then the financial effect shows up. Better first-pass authorization performance usually means fewer held claims, fewer post-service write-offs tied to medical necessity disputes, and less staff labor spent on preventable appeals.
Clinical and financial effects you can actually feel
The strongest systems improve daily operations in ways a clinic can track:
- More predictable scheduling. Procedure slots are less likely to be reserved for services still waiting on payer review.
- Cleaner downstream claims. Requests that match the chart and planned service create fewer billing contradictions later.
- Lower rework per case. Staff are not reopening the same chart to add wound duration, failed standard care, or missing measurements after the payer asks for them.
- Clearer denial patterns. Repeated failures by payer, service line, or documentation element become visible, so managers can fix the intake or charting process upstream.
Wound clinics should judge these systems the same way they judge any other operational purchase. Do they reduce time to treatment? Do they reduce avoidable denials? Do they protect revenue for high-scrutiny services such as surgical debridement and skin substitutes? If the answer is yes, the software is doing real work.
There is also a direct connection between authorization quality and payment performance. Clinics trying to reduce rework after the visit should look at how prior auth data feeds the broader healthcare claims management workflow. A weak request often becomes a weak claim, especially when the procedure note, diagnosis coding, and supporting wound history do not line up.
Case Files From the Clinic
The difference between helpful software and decorative software shows up in real denials. Two examples come up over and over in wound practices.
Case one with a skin substitute appeal
A non-healing lower extremity wound had already gone through standard care, serial debridement, moisture balance, and offloading. The request for a skin substitute was denied anyway. The payer reviewer said progression wasn't adequately documented.
The failure point wasn't the clinical plan. It was the appeal package. The chart had photos, but they weren't organized to show wound trajectory clearly. Measurements existed, but they lived across separate visits and weren't assembled into a quick visual record.
That's where software with image analysis and archived wound trajectory becomes more than a convenience. A 2024 PMC study found that peer-to-peer processes consume 3.2 hours per case but resolve only 34% of denials because reviewers often lack access to original wound trajectory data, such as surface area change over time. Automated image analysis provides this missing evidence, according to this peer-to-peer denial analysis in wound care.
In practical terms, that means an appeal works better when you can show serial wound area change, annotated images, tissue transition, and timing of prior treatment in one package. The clinician arguing the appeal needs evidence, not memory.
Case two with a debridement note saved before submission
This one never became a denial because the problem was caught early. The physician dictated a note for debridement and documented “slough in wound bed with moderate drainage.” Clinically, that's familiar language. Administratively, it's thin.
The software flagged the note before submission because it lacked the specifics needed to support the selected debridement code and the payer's medical necessity standard. The revised note added:
- Percentage of slough present
- Depth reached during debridement
- Exudate type, such as serosanguinous rather than generic drainage
- Periwound findings and whether maceration or erythema was present
- Updated measurements tied to the encounter
The best denial is the one your team never has to fight because the note was corrected while the patient was still in the room.
That's the kind of prevention busy clinics need. Not another dashboard. A system that catches “too vague to bill safely” before the request gets sent.
An Evaluation Checklist for Prior Authorization Software
Most clinics don't need more features. They need fewer blind spots. If you're evaluating prior authorization software for wound care, ask whether it handles the exact places your denials start: incomplete wound descriptors, fragmented data, unsupported code selection, and missing authorization details on the claim side.
What to ask before you buy
| Evaluation Category | Key Question for Vendor |
|---|---|
| EHR workflow fit | Does it work inside the existing task queue, or will staff have to re-enter data in another portal? |
| Wound note parsing | Can it read unstructured wound details such as slough percentage, exudate type, periwound condition, and depth from dictated or typed notes? |
| Code support | Does it align documentation with wound-relevant CPT codes such as 11042 through 11047 and the related ICD-10-CM diagnoses used in your clinic? |
| Advanced therapy logic | Can it flag missing support for NPWT, skin substitutes, and other high-scrutiny wound services before submission? |
| Image and measurement handling | Does it organize serial wound images and measurements in a form that supports appeals and re-review? |
| Human review path | When confidence is low or the case is unusual, does it escalate to staff review instead of submitting a weak request? |
| Payer rule maintenance | Who updates the payer rules, and how quickly are changes reflected in the workflow? |
| Claim handoff | Does the authorization number flow correctly into billing so approved services don't fail later at claim submission? |
| Audit trail | Can you see exactly what data supported the request and who edited it before submission? |
| Reporting | Can the clinic track denial themes by payer, service line, and documentation gap? |
One billing detail that still sinks clean cases
For wound graft prior authorization submitted on the CMS-1500 form, a valid authorization number must be documented in Field 23; without it, claims are denied regardless of the quality of the supporting clinical documentation, as explained in this wound graft prior authorization billing reference.
That's a useful litmus test when you evaluate any system. Ask the vendor to show exactly how the authorization number reaches Field 23. Don't accept “it integrates with billing” as the answer.
A low-risk rollout plan
A sensible implementation doesn't start with every payer and every procedure.
- Start with one high-friction service. NPWT or skin substitutes are common places to begin.
- Limit the first phase to one payer group. You'll learn faster with a narrower rule set.
- Audit notes weekly at the start. Look for repeated gaps in slough percentage, wound depth, prior standard care, and measurements.
- Train clinicians on documentation triggers, not software menus. Staff adoption rises when the lesson is about avoiding denials, not clicking buttons.
If the system can't make wound documentation cleaner, more complete, and easier to defend, it won't help for long.
Wound clinics don't need another generic tech layer. They need documentation, coding, image analysis, and prior authorization support that matches how wound care is practiced and paid. EkagraHealth AI is built for that reality, with clinician-founded workflows that help teams capture the right wound details, support cleaner CPT and ICD-10-CM selection, organize image-based evidence, and keep prior auths and claims from stalling revenue.
